Related Subjects:
|Anatomy of Skin
|Anatomy of the Hand
|Anatomy of the Thorax
|Anatomy of Muscle Groups
|Anatomy of Anatomy of Arteries
|Anatomy of Spinal Column
|AP of the Cerebrum
🧠 AP of the Cerebral Cortex
Structure of the Cerebrum
The cerebrum is the largest part of the human brain and underpins higher functions including thought, language, executive control, voluntary movement, and conscious sensory perception. Its outer sheet-the cerebral cortex-is a densely organised network of neurons and glial cells arranged into layers and columns, allowing rapid integration of information across multiple regions. Beneath the cortex lies white matter (myelinated axons) connecting cortical areas to each other and to subcortical structures.
The cortex works as a predictive, integrative processor: it combines incoming sensory signals with prior experience, selects actions, and continuously updates internal models of the world. Many clinical syndromes (stroke, epilepsy, dementia, delirium) can be understood as disruption of specific cortical networks.
Neurons
Neurons are the brain’s primary information-processing units, communicating via electrical activity (action potentials) and chemical synapses. The cerebral cortex contains several neuronal classes arranged into six layers (I–VI). Broadly, pyramidal neurons provide long-range excitatory output (glutamatergic), while interneurons provide local inhibitory control (GABAergic) that shapes timing, synchrony, and stability of cortical activity.
- Pyramidal Cells
- Shape: Pyramid-shaped soma with a long apical dendrite extending toward the cortical surface and basal dendrites spreading horizontally.
- Function: Major excitatory neurons driving cognition, motor planning, and long-range cortico-cortical and cortico-subcortical communication (glutamate).
- Location: Prominent in layers III and V; layer III supports association/commissural outputs, layer V supports descending outputs.
- Stellate Cells
- Shape: Star-shaped with multiple dendritic branches.
- Function: Often specialised for processing incoming sensory information and relaying it locally within cortical circuits; can be excitatory or inhibitory depending on subtype.
- Location: Classically enriched in layer IV, especially in primary sensory cortices (strong thalamic input).
- Betz Cells
- Shape: Very large pyramidal neurons.
- Function: Powerful descending output for motor control; contribute to corticospinal pathways involved in voluntary movement.
- Location: Layer V of the primary motor cortex (precentral gyrus).
- Interneurons
- Function: Primarily inhibitory (GABA) neurons that gate excitation, sculpt receptive fields, and stabilise networks to prevent runaway firing (key in epilepsy physiology).
- Types: Basket cells, chandelier cells, double bouquet cells, and others-each with characteristic connectivity and timing effects.
- Location: Distributed across all cortical layers.
Glial Cells
Glial cells (neuroglia) support and regulate neuronal function. They maintain ionic and metabolic homeostasis, modulate synaptic transmission, form myelin, provide immune surveillance, and contribute to cerebrospinal fluid dynamics. Many neurological diseases involve glia (e.g., demyelination, neuroinflammation, tumour biology).
- Astrocytes
- Function: Support synapses and neurons, buffer extracellular potassium, recycle neurotransmitters (e.g., glutamate), regulate blood flow (neurovascular coupling), and maintain the blood–brain barrier.
- Clinical link: Astrocytic dysfunction contributes to cerebral oedema, excitotoxicity, and seizure susceptibility.
- Location: Throughout CNS (grey and white matter).
- Oligodendrocytes
- Function: Produce myelin in the CNS, enabling rapid saltatory conduction and efficient long-range connectivity.
- Clinical link: Demyelination (e.g., MS) causes slowed conduction and “disconnection” syndromes.
- Location: Predominantly white matter, also present in grey matter.
- Microglia
- Function: Resident immune cells; phagocytose debris/pathogens, prune synapses during development, and orchestrate inflammatory signalling.
- Clinical link: Overactivation contributes to neuroinflammation in infection, stroke, and neurodegenerative disorders.
- Location: Throughout CNS.
- Ependymal Cells
- Function: Line ventricles and central canal; cilia help circulate CSF; related specialised epithelium in choroid plexus produces CSF.
- Clinical link: Disrupted CSF flow dynamics contribute to hydrocephalus physiology.
- Location: Ventricular system and central canal.
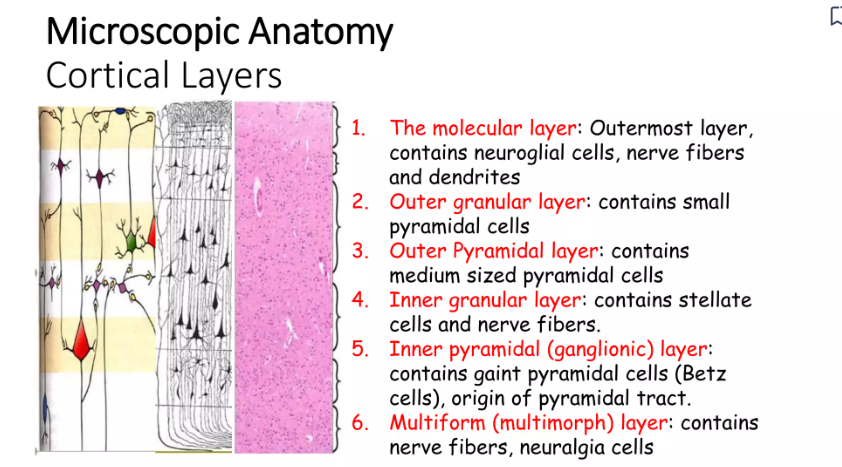
Layered Organization of the Cerebral Cortex
The neocortex is organised into six layers. The pattern of thickness and cellular density varies by region (e.g., motor vs sensory cortex), reflecting differences in input–output demands.
- Layer I – Molecular Layer: Few neuronal bodies; rich in dendrites/axons → intracortical integration.
- Layer II – External Granular Layer: Small pyramidal/stellate neurons; local cortical processing and short-range connections.
- Layer III – External Pyramidal Layer: Medium pyramidal neurons; outputs to other cortical regions (association fibres) and across hemispheres (commissural fibres via corpus callosum).
- Layer IV – Internal Granular Layer: Dense stellate neurons; major recipient of thalamocortical sensory input (prominent in sensory cortex).
- Layer V – Internal Pyramidal Layer: Large pyramidal neurons (including Betz cells); outputs to brainstem/spinal cord and other subcortical targets.
- Layer VI – Multiform Layer: Diverse neurons; outputs to thalamus and forms feedback loops controlling thalamic gating.
Regional specialisation: Primary sensory cortex has a prominent Layer IV (heavy thalamic input), whereas primary motor cortex has a prominent Layer V (strong descending output).
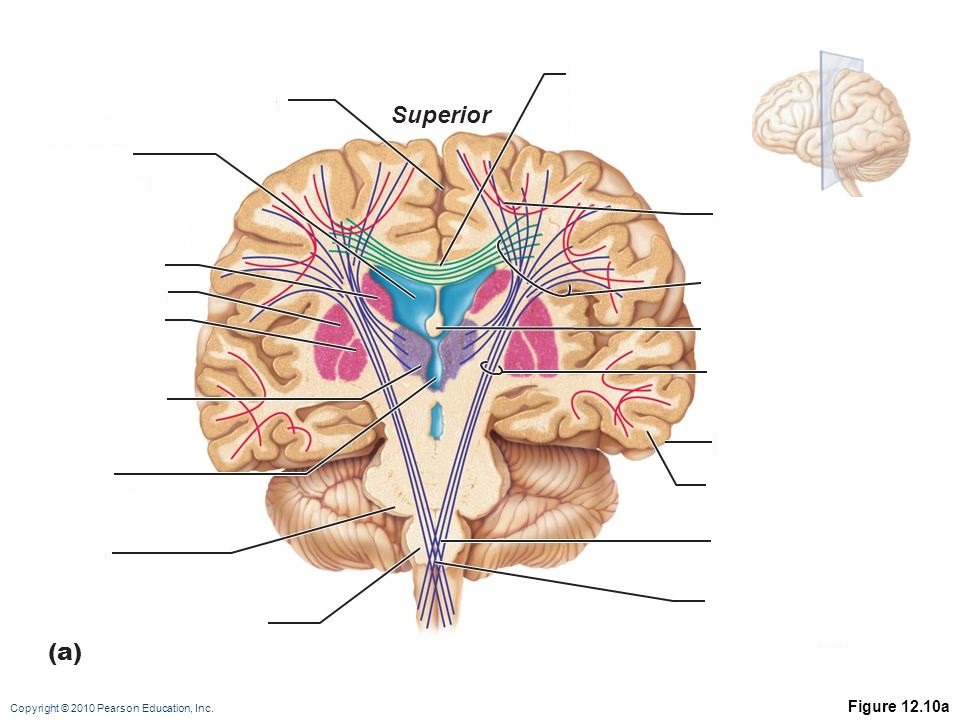
Columnar Organization and Connectivity
Beyond layers, cortex is arranged in columns-vertical processing units that share inputs and outputs (e.g., ocular dominance columns in visual cortex). Information flows through recurrent loops: thalamus → layer IV → layers II/III → layers V/VI, with extensive feedback and lateral connectivity. White matter pathways include association fibres (same hemisphere), commissural fibres (corpus callosum), and projection fibres (internal capsule to/from brainstem/spinal cord).
Physiology: How the Cortex Processes Information
- Excitation–inhibition balance: Pyramidal excitation is tightly regulated by GABAergic interneurons to prevent runaway firing. Disruption predisposes to seizures.
- Synaptic plasticity: Cortical circuits change with experience (LTP/LTD), underpinning learning, memory, and rehabilitation after injury.
- Oscillations and synchrony: Interneurons help generate rhythms (alpha/beta/gamma) important for attention, perception, and coordinated motor output.
- Neurovascular coupling: Astrocytes and vascular signals match blood flow to neuronal activity (basis of fMRI and “perfusion demand”).
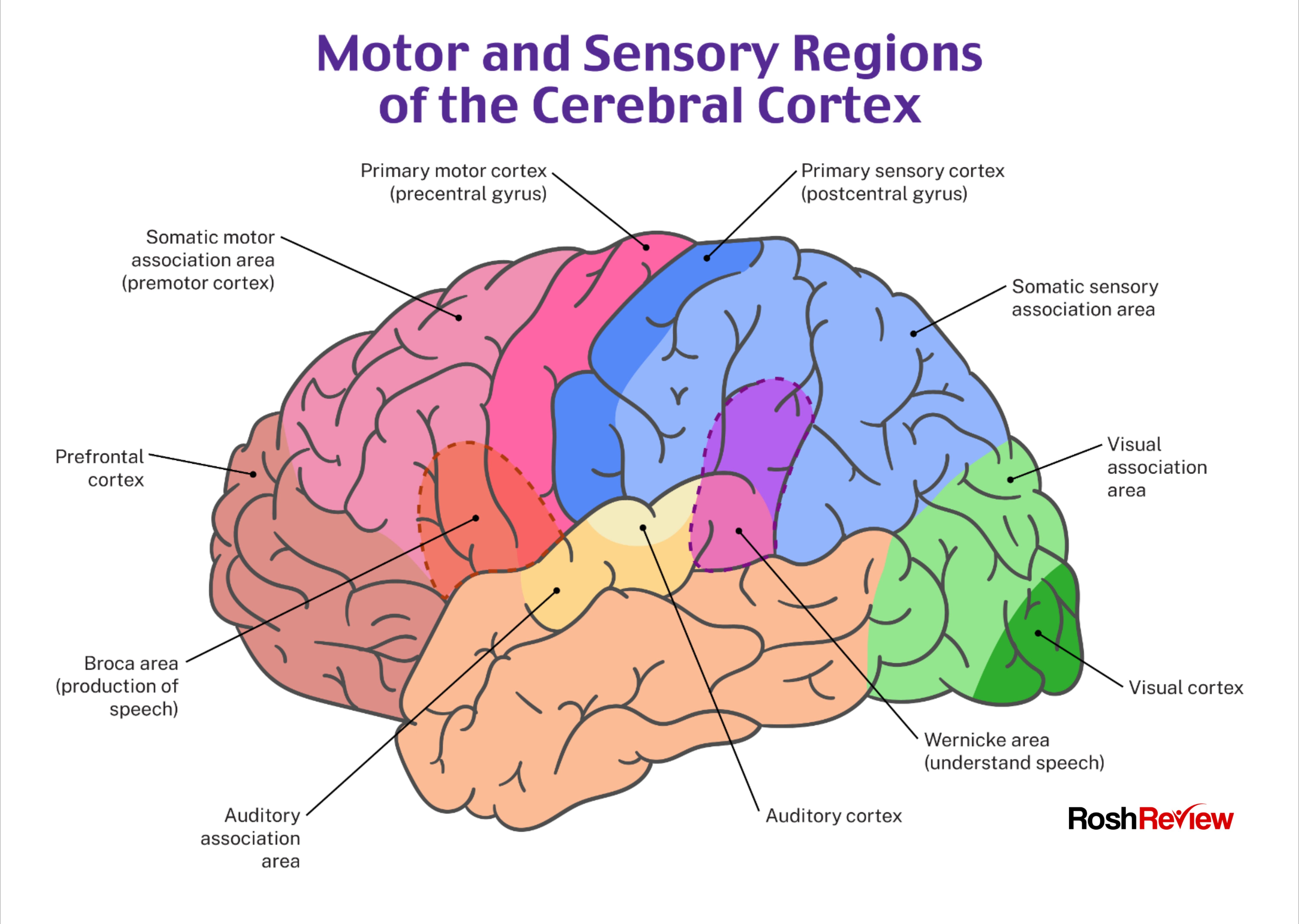
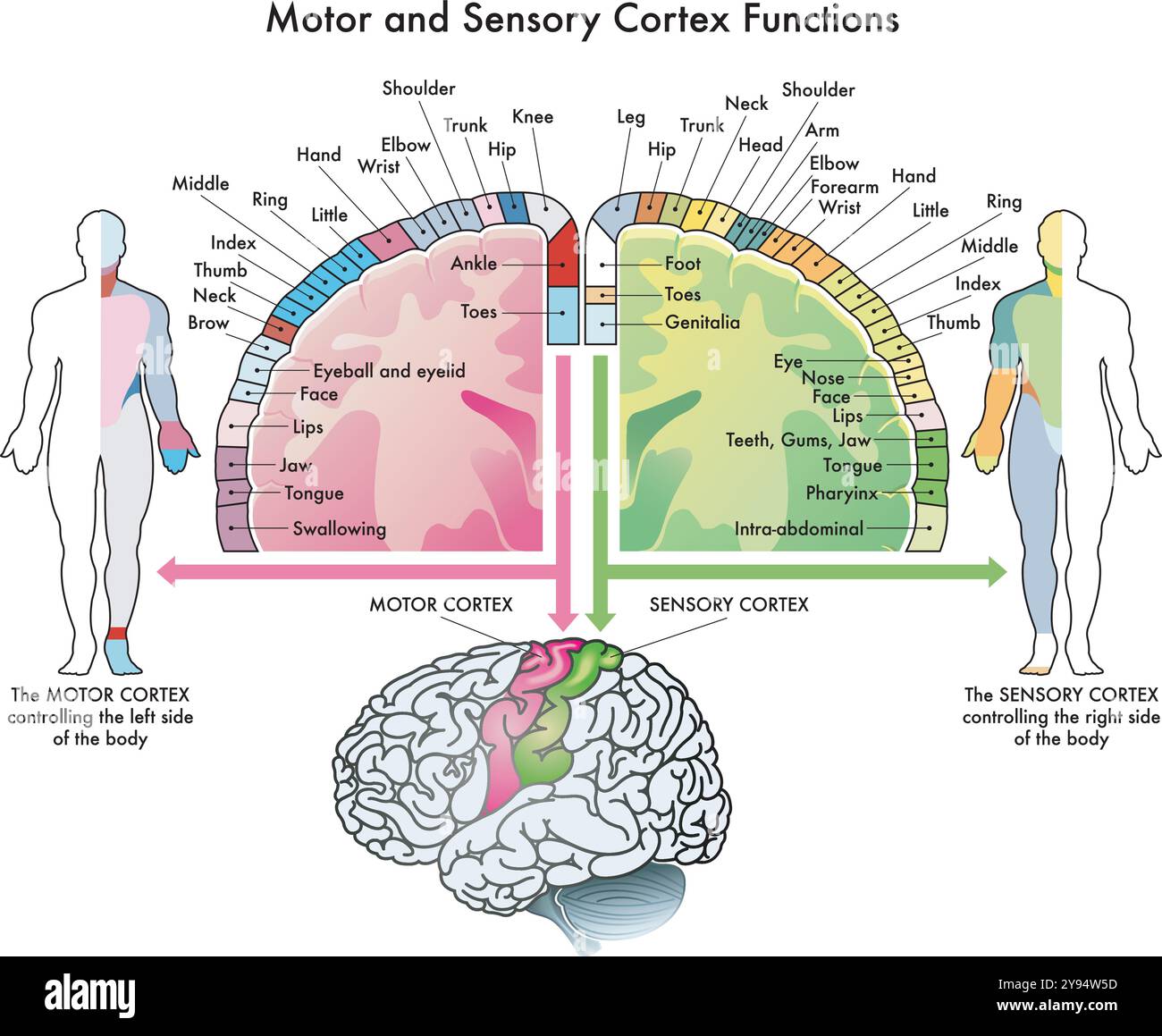
Functional Significance
- Sensory Processing: Primary sensory cortices receive thalamic input (Layer IV) and construct conscious perception; association cortices integrate meaning and context.
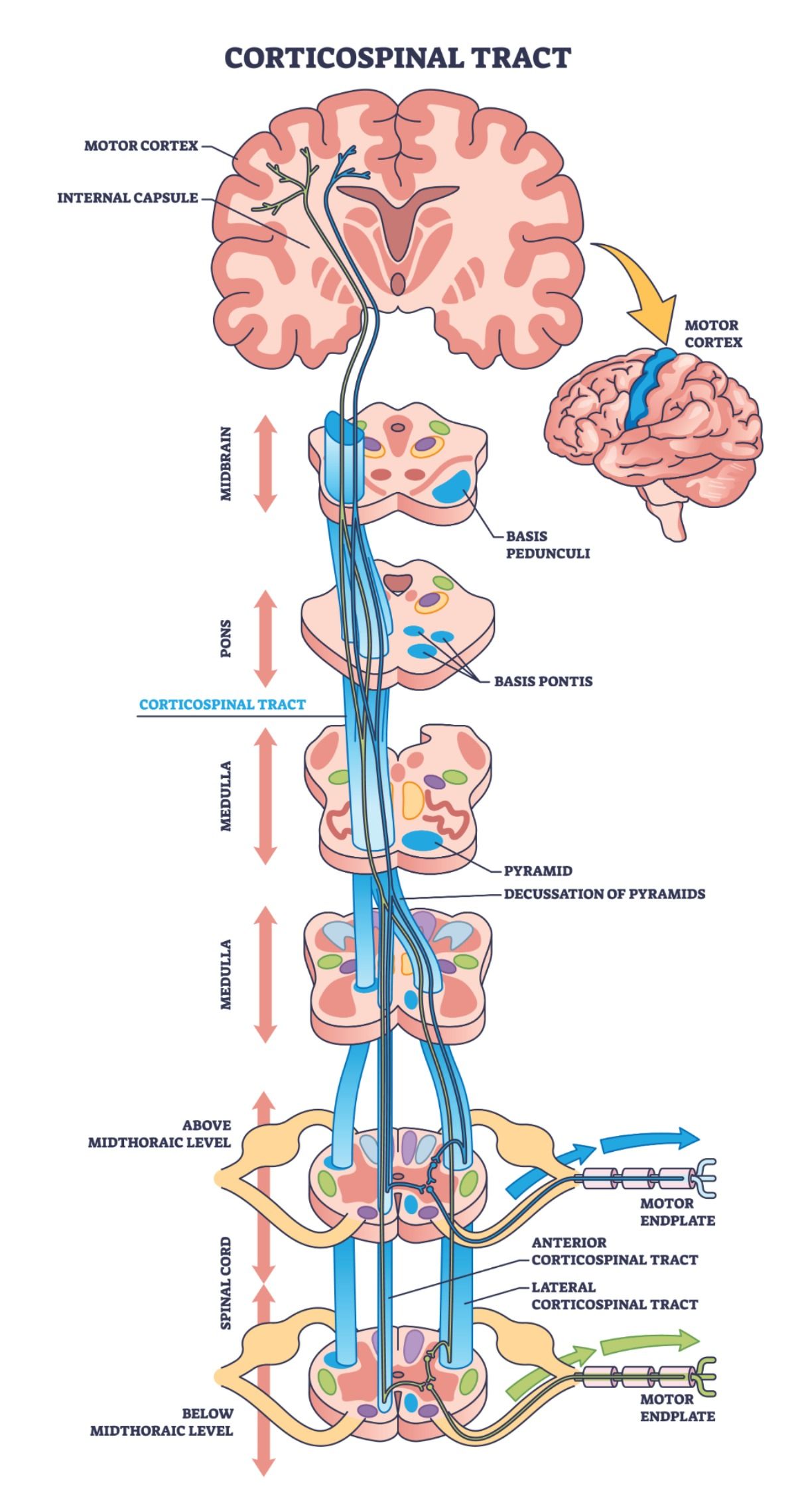
- Motor Control: Motor cortex (Layer V outputs) initiates voluntary movement through corticospinal and corticobulbar pathways; premotor areas plan sequences.
- Cognition and Language: Fronto-parietal and temporal association networks support working memory, decision-making, attention, and language.
- Support and Protection: Glia maintain homeostasis, myelin, immune surveillance, and CSF dynamics-essential for stable cortical function.
🩺 Clinical Relevance (high-yield)
- Stroke syndromes: Focal deficits reflect cortical localisation (e.g., MCA infarct → aphasia or neglect depending on hemisphere; homonymous hemianopia with occipital involvement).
- Epilepsy: Cortical hyperexcitability often arises from altered inhibition, gliosis, or structural lesions; EEG reflects abnormal synchrony.
- Demyelination: Oligodendrocyte injury disrupts white matter “wiring”, producing sensory, motor, and cognitive disconnection symptoms.
- Neurodegeneration: Network failure in association cortices explains progressive cognitive syndromes (e.g., Alzheimer’s).
Conclusion
The cerebral cortex is a layered and columnar network built from excitatory pyramidal neurons, diverse inhibitory interneurons, and essential supporting glial cells. Layers I–VI provide a structured route for thalamic input, intracortical integration, and descending output, with regional specialisation in sensory and motor areas. Glia maintain the chemical, metabolic, and immune environment needed for stable signalling and plasticity. This cellular architecture enables conscious sensation, voluntary movement, language, and higher cognition-and explains why focal lesions or network dysfunction produce recognisable neurological syndromes.
🗺️ Brodmann Areas and Cortical Localisation
The cerebral cortex can be subdivided into Brodmann areas based on differences in cellular architecture (cytoarchitecture). These regions, described by Korbinian Brodmann, correlate closely with functional specialisation and remain highly relevant in neurology, stroke medicine, neurosurgery, and neuroimaging.
Brodmann areas link microscopic structure to clinical function. Focal lesions often produce predictable deficits because specific functions are concentrated within defined cortical territories.
- Primary cortices receive or generate direct sensory/motor signals.
- Secondary areas refine and interpret information.
- Association areas integrate multimodal input for cognition, language, and behaviour.
📊 Key Brodmann Areas: Anatomy and Function
| Brodmann Area |
Anatomical Location |
Primary Function |
Clinical Correlation |
| 4 |
Precentral gyrus (frontal lobe) |
Primary motor cortex - voluntary movement |
Contralateral weakness/paralysis (UMN signs) |
| 6 |
Premotor & supplementary motor cortex |
Motor planning and coordination |
Apraxia, impaired motor sequencing |
| 1, 2, 3 |
Postcentral gyrus (parietal lobe) |
Primary somatosensory cortex |
Contralateral sensory loss, impaired proprioception |
| 5, 7 |
Superior parietal lobule |
Sensory integration, spatial awareness |
Neglect, visuospatial deficits |
| 17 |
Calcarine cortex (occipital lobe) |
Primary visual cortex (V1) |
Contralateral homonymous hemianopia |
| 18, 19 |
Occipital lobe (visual association) |
Visual interpretation and recognition |
Visual agnosia, perceptual deficits |
| 41, 42 |
Superior temporal gyrus |
Primary auditory cortex |
Auditory processing deficits |
| 22 |
Posterior superior temporal gyrus |
Language comprehension (Wernicke’s area) |
Receptive aphasia |
| 44, 45 |
Inferior frontal gyrus (dominant hemisphere) |
Language production (Broca’s area) |
Expressive aphasia |
| 8 |
Frontal eye fields |
Voluntary eye movements |
Gaze deviation toward lesion |
| 9, 10, 11, 12, 46, 47 |
Prefrontal cortex |
Executive function, judgement, behaviour |
Disinhibition, personality change, poor planning |
| 20, 21, 37 |
Inferior temporal cortex |
Object and face recognition |
Visual agnosia, prosopagnosia |
| 23, 24, 31, 32 |
Cingulate cortex |
Emotion, motivation, attention |
Apathy, emotional dysregulation |
| 28, 34 |
Entorhinal cortex (medial temporal) |
Memory processing (hippocampal gateway) |
Early impairment in Alzheimer’s disease |
🧠 Functional Networks and Brodmann Areas
Although Brodmann areas describe discrete regions, most higher functions arise from distributed networks. For example:
- Language: Areas 44/45 (production) + 22 (comprehension) + arcuate fasciculus.
- Vision: Area 17 → 18/19 → temporal/parietal streams.
- Executive control: Prefrontal areas interacting with basal ganglia and thalamus.
- Motor control: Areas 4/6 integrated with cerebellum and brainstem.
Modern imaging shows that Brodmann areas act as “nodes” within large-scale networks. Stroke, tumour, or neurodegeneration disrupts both the local cortex and its long-range connections.
✅ Makindo Exam & Clinical Pearls - Brodmann Areas
- Area 4 = movement, 1–3 = sensation, 17 = vision.
- 44/45 = Broca, 22 = Wernicke (dominant hemisphere).
- Frontal eye fields (8) → gaze toward lesion in acute stroke.
- Prefrontal damage → behavioural and executive dysfunction.
- Parietal association damage → neglect (usually right hemisphere).
