
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Erythrocytes / Red Blood Cells 🩸
Related Subjects: |Heme |Globins |Red blood cells |White blood cells |Lymphocytes |Platelets |Cryoprecipitate |Fresh Frozen Plasma |Blood Cell Maturation |Blood film interpretation |Reticulocytes
🩸 Erythrocytes, also known as red blood cells (RBCs), are the most abundant cells in the blood. Their main role is to transport oxygen from the lungs to the tissues and to help return carbon dioxide from the tissues to the lungs for exhalation. 💡 They are highly specialised cells, designed to maximise gas transport while remaining flexible enough to pass through tiny capillaries.
🩸 Structure of Red Blood Cells
- 🔴 Biconcave disc shape
- Increases surface area for efficient gas exchange.
- Creates a short diffusion distance for oxygen and carbon dioxide.
- Provides the flexibility needed to pass through narrow capillaries and splenic sinusoids.
- 🧬 No nucleus or organelles in mature RBCs
- Maximises space for haemoglobin.
- Prevents the cell from using the oxygen it is carrying.
- Means mature RBCs cannot divide or synthesise new proteins, limiting their lifespan.
- 🫁 Haemoglobin is the major intracellular protein
- Each haemoglobin molecule contains 4 globin chains and 4 haem groups.
- Each haem group contains an iron atom that binds 1 oxygen molecule.
- Therefore, each haemoglobin molecule can carry up to 4 oxygen molecules.
⚙️ Functions of Red Blood Cells
- 🫁 Oxygen transport
- RBCs pick up oxygen in the lungs, where oxygen binds reversibly to haemoglobin.
- They deliver oxygen to tissues, where it is released for cellular respiration.
- 🌬️ Carbon dioxide transport
- RBCs help remove carbon dioxide, a waste product of metabolism, from tissues.
- Carbon dioxide is carried in 3 forms:
- Dissolved in plasma
- As bicarbonate (HCO3−) after conversion inside RBCs by carbonic anhydrase
- Bound to haemoglobin as carbaminohaemoglobin
- ⚖️ Buffering blood pH
- Haemoglobin helps buffer hydrogen ions (H+), contributing to acid–base balance.
- This is one reason RBCs are important not only for gas transport, but also for overall physiological stability.
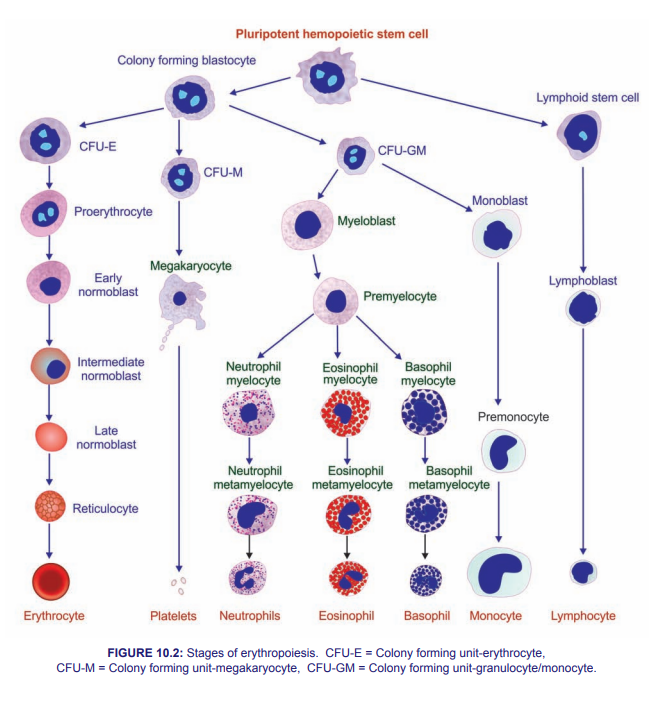
🏭 Erythropoiesis
- Erythropoiesis is the process of red blood cell production.
- 📍 It occurs in the bone marrow.
- 🧪 It is stimulated by erythropoietin (EPO), a hormone produced mainly by the kidneys in response to hypoxia.
- 📈 Main stages of development:
- Haematopoietic stem cell
- Erythroid progenitor cell
- Proerythroblast
- Erythroblast
- Reticulocyte
- Mature erythrocyte
- 🟣 Reticulocytes are immature RBCs that still contain a small amount of residual RNA and usually mature in the bloodstream within 1–2 days.
⏳ Life Cycle of Red Blood Cells
- RBCs survive for approximately 120 days.
- Old or damaged RBCs are removed by macrophages in the:
- Spleen
- Liver
- Bone marrow
- 🧪 Haemoglobin is broken down into:
- Globin → amino acids for reuse
- Haem → iron + protoporphyrin
- Iron is recycled
- Biliverdin is converted to bilirubin, which is excreted in bile
🩺 Clinical Relevance of Red Blood Cells
- 📉 Anaemia
- Reduced number of RBCs or reduced haemoglobin concentration lowers oxygen-carrying capacity.
- Causes include:
- Iron deficiency
- Vitamin B12 or folate deficiency
- Chronic disease
- Haemoglobinopathies such as sickle cell disease or thalassaemia
- Symptoms include fatigue, pallor, breathlessness, dizziness, and reduced exercise tolerance.
- 📈 Polycythaemia
- An increased RBC mass raises blood viscosity and increases thrombotic risk.
- May be:
- Primary - e.g. polycythaemia vera
- Secondary - e.g. chronic hypoxia or excess EPO production
- 💥 Haemolytic disorders
- RBC destruction exceeds bone marrow production.
- Causes include:
- Autoimmune haemolysis
- Infections
- Drugs
- Membrane defects
- Enzyme deficiencies such as G6PD deficiency
🌟 Summary
🩸 Red blood cells are highly specialised cells designed for oxygen delivery, carbon dioxide transport, and acid–base buffering. Their biconcave shape, lack of nucleus, and high haemoglobin content make them ideally suited to this role. Understanding their structure, production, lifespan, and pathology is essential for recognising common haematological disorders.
🧱 Overview of the Red Cell Membrane
🧩 The red cell membrane is a dynamic structure that gives RBCs the strength, flexibility, and deformability needed to survive repeated passage through the circulation and spleen. It is crucial for maintaining the normal biconcave shape and preventing premature haemolysis.
🧬 Structure of the Red Cell Membrane
- The membrane consists of:
- 🧈 Lipid bilayer
- 🔗 Membrane proteins
- 🕸️ Cytoskeletal network
- 🧈 Lipid bilayer
- Made of phospholipids, cholesterol, and glycolipids.
- Forms a semi-permeable barrier controlling entry and exit of ions and water.
- Hydrophilic heads face outward; hydrophobic tails face inward.
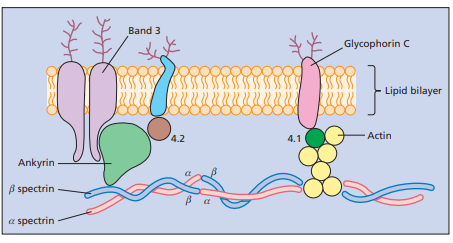
- 🔗 Membrane proteins
- Integral proteins span the membrane.
- Peripheral proteins attach to the membrane surface and cytoskeleton.
- Important integral proteins include:
- Band 3 - chloride/bicarbonate exchanger, important in CO₂ transport
- Glycophorin - contributes negative surface charge and reduces cell aggregation
- Important peripheral/cytoskeletal proteins include:
- Spectrin - major structural scaffold
- Actin - supports membrane stability
- Ankyrin - anchors spectrin to Band 3
- Protein 4.1 and Protein 4.2 - strengthen membrane-cytoskeleton interactions
- 🕸️ Cytoskeletal network
- Mainly composed of spectrin, actin, and associated proteins.
- Provides durability while allowing the RBC to deform dramatically without rupturing.
⚙️ Functions of the Red Cell Membrane
- 🔴 Maintains cell shape and integrity
- Preserves the biconcave shape needed for optimal gas exchange.
- Helps the RBC tolerate mechanical stress in the circulation.
- 🤸 Deformability
- Allows RBCs to squeeze through capillaries smaller than their resting diameter.
- Essential for survival during splenic filtration.
- 🚪 Selective permeability
- Regulates movement of ions and water.
- Maintains osmotic balance and cell volume.
- 🛡️ Surface protection
- Negative charge from sialic acid residues helps prevent RBCs from sticking together.
- Supports normal circulation and reduces unwanted aggregation.
- 📡 Functional interactions
- Membrane proteins are involved in transport, structural support, and cell survival.
🩺 Clinical Relevance of the Red Cell Membrane
- ⚪ Hereditary spherocytosis
- Usually due to defects in spectrin, ankyrin, Band 3, or protein 4.2.
- RBCs become spherical, less deformable, and are removed by the spleen.
- Features include anaemia, jaundice, splenomegaly, and gallstones.
- 🥚 Hereditary elliptocytosis
- Usually caused by abnormalities in spectrin or related cytoskeletal proteins.
- RBCs become elliptical and may haemolyse in more severe cases.
- 🌙 Paroxysmal nocturnal haemoglobinuria (PNH)
- An acquired stem cell disorder caused by a PIGA mutation.
- Leads to deficiency of GPI-anchored proteins such as CD55 and CD59.
- This makes RBCs vulnerable to complement-mediated lysis.
- Classically associated with haemolysis, haemoglobinuria, thrombosis, and marrow failure.
- 🔥 Autoimmune haemolytic anaemia (AIHA)
- Antibodies target red cell surface antigens.
- Leads to premature RBC destruction, usually in the spleen and liver.
- Features include anaemia, jaundice, and sometimes splenomegaly.
🌟 Final Summary
🩸 Red cells are beautifully specialised cells built for gas transport, while the red cell membrane gives them the strength and flexibility needed to survive in circulation. 🧬 The membrane is made of a lipid bilayer, integral proteins, and a spectrin-based cytoskeleton. ⚠️ Disorders of haemoglobin, membrane proteins, enzymes, or immune attack can all shorten RBC survival and cause haemolytic anaemia.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery