Humeral Fractures ✅
Humeral Fractures: ⚠️ If there are neurological deficits (wrist/hand weakness, sensory loss), vascular compromise (absent/distal pulses, pallor), or involvement of the shoulder/elbow joints → urgent orthopaedic referral is required.
📖 About
- Humeral fractures are common after FOOSH (fall onto an outstretched hand) in older adults; younger patients often sustain fractures from direct trauma.
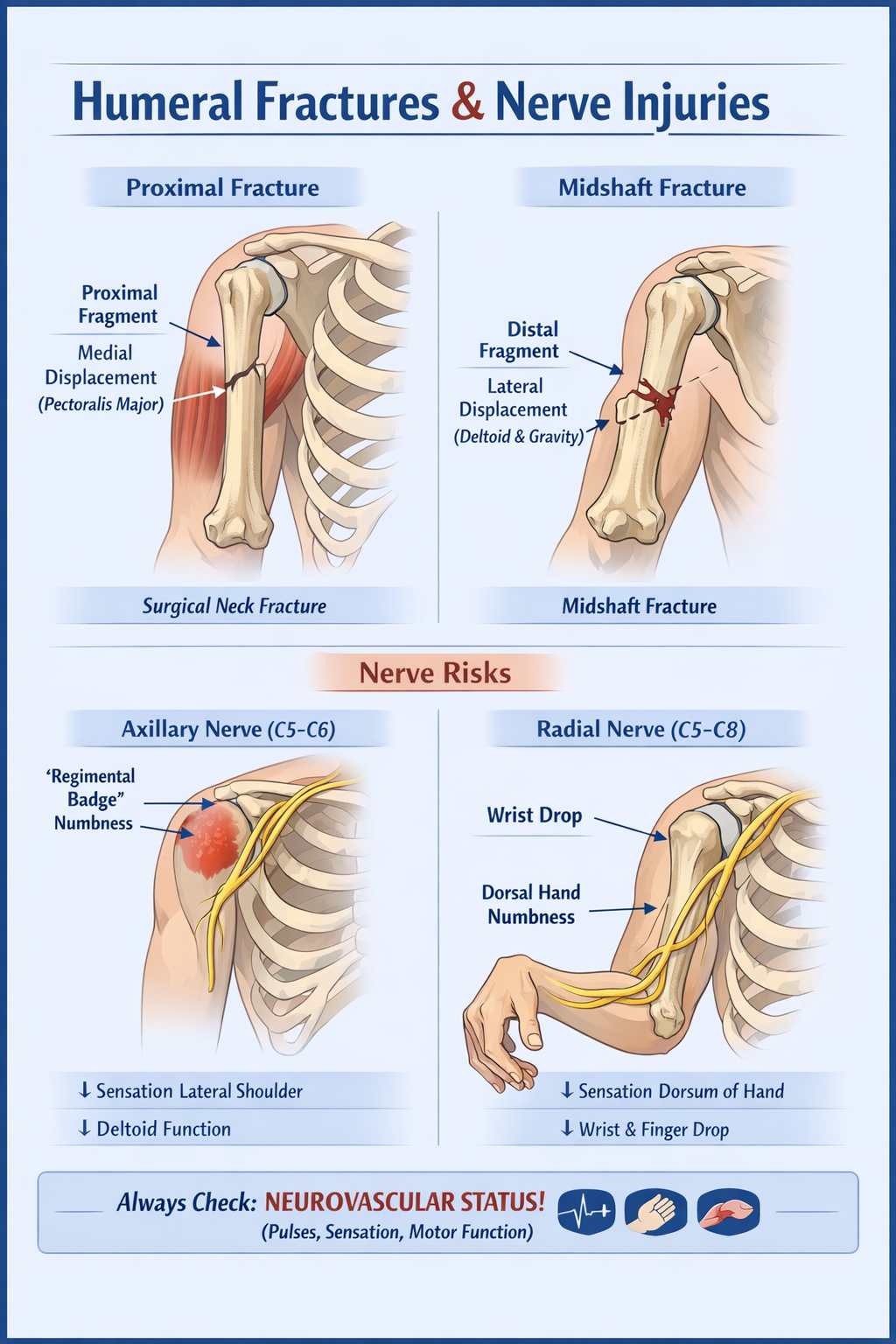
- Proximal third fractures: proximal fragment pulled medially by pectoralis major.
- Midshaft fractures: distal fragment abducted by deltoid, may also be affected by gravity.
- Distal fractures may involve supracondylar region or condyles, impacting elbow function.
🧾 Aetiology
- Trauma (falls, sports injuries, RTCs) – most common.
- Pathological bone: osteoporosis, Paget’s disease, metastatic lesions.
- Mechanism: FOOSH, direct blow, twisting injury.
- Fracture sites: anatomical or surgical neck, greater/lesser tuberosity, midshaft, distal humerus.
🩺 Clinical Features
- Severe pain, swelling, tenderness, bruising; limb may be supported by opposite hand.
- Deformity, angulation, or shortening may be present.
- Radial nerve injury: wrist/hand drop, dorsum sensory loss (runs in spiral groove of midshaft).
- Axillary nerve injury: loss of sensation over “regimental badge” area, weak shoulder abduction.
- Always assess brachial plexus function, distal pulses, and perfusion.
- Look for open wounds → risk of compound fracture and infection.
🔍 Investigations
- Bloods: FBC, ESR, U&E, calcium (to rule out pathological cause in older adults).
- X-rays: AP + lateral views of humerus; include axillary or Y view for proximal fractures.
- CT: indicated for complex, comminuted, intra-articular fractures, or pre-operative planning.
- Consider neurovascular imaging if pulse deficit or suspected brachial artery injury.
⚠️ Complications
- Radial nerve palsy (~10–18% of midshaft fractures).
- Open/compound fractures → infection risk.
- Malunion, non-union, or delayed union (higher in pathological bone).
- Shoulder stiffness or rotator cuff injury after proximal humeral fractures.
- Volkmann’s ischaemic contracture (rare in distal humerus fractures with vascular compromise).
🛠️ Management
- Urgent orthopaedic referral if:
- Gross displacement, angulation, or comminution
- Open/compound fracture
- Radial or brachial nerve palsy
- Vascular compromise (absent distal pulse, pallor, cold limb)
- Joint involvement (shoulder/elbow)
- Otherwise (non-displaced or minimally displaced):
- Immobilisation: U-slab plaster or hanging cast; pad well.
- Analgesia: paracetamol ± opioids for severe pain; consider NSAIDs if no contraindications.
- Early mobilisation of fingers and shoulder/elbow as tolerated to prevent stiffness.
- Arrange fracture clinic review within 1 week for reassessment and possible imaging.
- Physiotherapy input post-immobilisation to restore range of motion.
📚 References
- Rockwood & Green’s Fractures in Adults, 9th Edition
- British Orthopaedic Association (BOA) Guidelines: BOA Guidelines
- RCSEng: Management of Upper Limb Fractures

