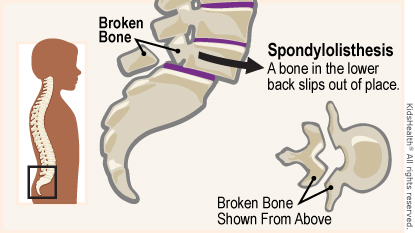
Spondylolisthesis
Related Subjects:
| Monoarticular Arthritis
| Polyarticular Arthritis
| Seronegative Spondyloarthropathies
| Ankylosing Spondylitis
| Enteropathic Spondyloarthritis
| Reactive Arthritis
| Psoriatic Arthritis
📖 About Spondylolisthesis
- Spondylolisthesis = forward displacement (slipping) of one vertebra over another, usually in the lumbar spine.
- Most commonly involves L4/L5 or L5/S1 vertebrae 🦴.
- Can cause spinal instability → chronic pain and, if severe, neurological deficits.
⚠️ Aetiology (Causes)
- Pars Interarticularis Defect (Spondylolysis) 🔨 – defect or stress fracture allows vertebral slip; classic in gymnasts, weightlifters, cricketers.
- Congenital (Dysplastic) 👶 – abnormal vertebral anatomy predisposes to early slip.
- Acquired / Degenerative 👵 – disc degeneration and facet arthritis in older adults.
- Trauma 🚑 – acute fracture leading to instability.
- Pathological 🦠 – e.g. tumour, infection, or metabolic bone disease.
🩺 Clinical Presentation
- Mechanical Low Back Pain 💢 – worsens with activity, eased by rest.
- Radicular Pain ⚡ – thigh/leg pain if nerve root compressed.
- Muscle Spasm 🤸 – paraspinal tightness, worsens later in day.
- Postural Change 🧍 – flattened lumbar lordosis, protuberant abdomen.
- Neurological Deficits ⚡ – numbness, weakness, gait disturbance (red flag 🚨).
- Severe cases: bladder/bowel dysfunction → urgent red flag referral for possible cauda equina.
🔎 Investigations
- Plain X-rays 📸 – lateral views show vertebral slip; oblique films may show “Scotty dog collar” (pars defect).
- MRI 🧲 – evaluates soft tissue, discs, nerve compression.
- CT scan 🖥️ – detailed bone anatomy, useful for surgical planning.
📊 Meyerding Grading (by % slip on lateral X-ray)
- I: 0–25% slip
- II: 26–50%
- III: 51–75%
- IV: 76–100%
- V: >100% (spondyloptosis)
💊 Management
- Conservative (Grades I–II, mild symptoms):
Analgesics, physiotherapy 🏃, core strengthening, posture/ergonomic advice, weight loss.
- Bracing (esp. adolescents with spondylolysis) may help reduce pain.
- Surgery (Grades III–V, failed conservative Rx, or neuro deficits):
Spinal fusion 🛠️ to stabilise and prevent progression.
- Minimally invasive options – selected cases for decompression + fusion.
- Long-term: Regular imaging, exercise, physio; avoid heavy impact sports if recurrent pain.
