Actinomyces israeli
🦠 Actinomyces israelii infection (actinomycosis) is a chronic suppurative disease that produces multiple abscesses and sinus tracts, often with discharge of characteristic yellow "sulfur granules" 🌾.
ℹ️ About
- 👨⚕️ First described by German surgeon James Adolf Israel in the 19th century.
- 🧫 Pathogen: Actinomyces israelii – a Gram-positive anaerobic bacterium, part of normal oral and gut flora.
- 🩺 Infection arises when mucosal barriers are disrupted (e.g. dental extraction, surgery, IUD insertion).
Characteristics
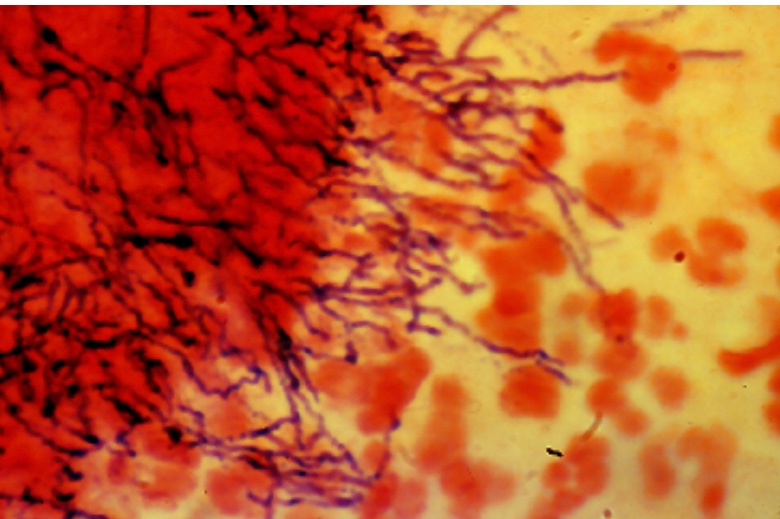
- 🔬 Gram-positive, branching, filamentous, non–acid-fast anaerobe.
- 🌾 Forms dense colonies producing sulfur granules, which are pathognomonic.
- 🎭 Often mimics malignancy due to invasive, destructive growth across tissue planes.
🧬 Aetiology
- ⚡ Opportunistic infection: Occurs in devitalised or traumatised tissue.
- 🦠 Main pathogen: Actinomyces israelii.
- 🦷 Common associations: poor oral hygiene, dental trauma, or long-term IUD use.

🩺 Clinical Features
- 👄 Cervicofacial actinomycosis ("lumpy jaw"):
- 🦷 Follows dental trauma or poor oral hygiene.
- 💊 Firm, painless swelling with multiple draining sinuses discharging sulfur granules.
- 🫁 Thoracic actinomycosis:
- Caused by aspiration, leading to lung/mediastinal abscesses.
- 🧠 Brain abscesses:
- Neurological deficits due to space-occupying lesions.
- 🩻 Abdominal/Pelvic actinomycosis:
- Often post-IUD insertion; pelvic pain, mass effect, chronic inflammation.
- 🔥 May mimic malignancy; fistulas and abscesses are common.
- Symptoms: abdominal pain, weight loss, fever, palpable mass.
🧪 Investigations
- 📋 Bloods: FBC may show anaemia of chronic disease, ↑WCC, raised ESR/CRP.
- 🩻 CXR: Cavitating, pleural-based, or mass-like lesions in thoracic actinomycosis; can mimic TB or lung cancer.
- 🖥️ Ultrasound/CT: Useful for abdominal/pelvic masses; helps detect fistulae or abscess spread across tissue planes.
- 🔬 Histology: “Sulphur granules” (yellow colonies) on microscopy are highly suggestive.
- 🥼 Culture: Anaerobic culture of pus/granules confirms diagnosis, but slow growth (may take 2–3 weeks).
💊 Management
- 💉 High-dose Penicillin G: First-line; usually IV for 2–6 weeks, then oral penicillin/amoxicillin for several months (total 6–12 months).
- 💊 Alternatives: Doxycycline, erythromycin, or clindamycin in penicillin-allergic patients (check BNF/local guidelines).
- 🔪 Surgery: Indicated for abscess drainage, fistula excision, or where malignancy is suspected (as Actinomyces can mimic tumours on imaging).
- 🩺 Follow-up: Long-term clinical and radiological monitoring needed, as relapse is common if treatment is stopped prematurely.
