
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Basal Ganglia
Related Subjects: |Brain Herniation syndromes |Haemorrhagic stroke |Traumatic Head/Brain Injury |Acute Hydrocephalus |Epidural Haematoma |Subdural haematoma |Basic Neuroscience |Medulla Oblongata |Midbrain |Pons |Caudate Nucleus |Putamen and Globus Pallidus |Cerebral Cortex |Internal Capsule |Cavernous sinus |Basal Ganglia
The basal ganglia are a group of interconnected subcortical nuclei embedded deep within the cerebral hemispheres and upper brainstem. They do not initiate movement directly; instead, they select, scale, and refine motor programmes generated by the cortex. Beyond movement, they are essential for procedural learning, habit formation, reward processing, and executive control.
Clinically, basal ganglia disorders produce characteristic movement syndromes (hypokinetic or hyperkinetic) because these nuclei regulate the balance between facilitation and inhibition of cortical motor output.
🏷️ Nuclei of the Basal Ganglia
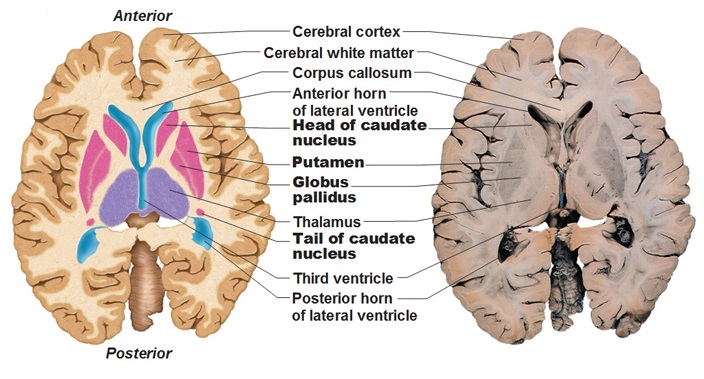
- Striatum (Input Nucleus)
- Composed of caudate nucleus + putamen.
- Main recipient of cortical glutamatergic input.
- Contains medium spiny neurons (GABAergic).
- Central to movement selection and learning.
- Putamen & Globus Pallidus (Lentiform Nucleus)
- Putamen: Motor control and execution.
- Globus pallidus:
- GPe: External segment (indirect pathway).
- GPi: Internal segment (major output nucleus).
- Caudate Nucleus
- C-shaped structure following the lateral ventricle.
- Involved in cognition, behavioural feedback, and goal-directed actions.
- Degeneration → chorea and cognitive decline (e.g. Huntington’s disease).
- Nucleus Accumbens (Ventral Striatum)
- Interface between limbic system and motor system.
- Central to reward, motivation, and addiction.
- Strong dopaminergic input from ventral tegmental area.
- Subthalamic Nucleus (STN)
- Excitatory (glutamatergic) nucleus.
- Key regulator of indirect pathway.
- Lesion → hemiballismus.
- Substantia Nigra
- Pars compacta (SNc): Dopamine → striatum.
- Pars reticulata (SNr): Output nucleus (similar to GPi).
The striatum receives information, the GPi/SNr send information out, and the remaining nuclei modulate this flow.
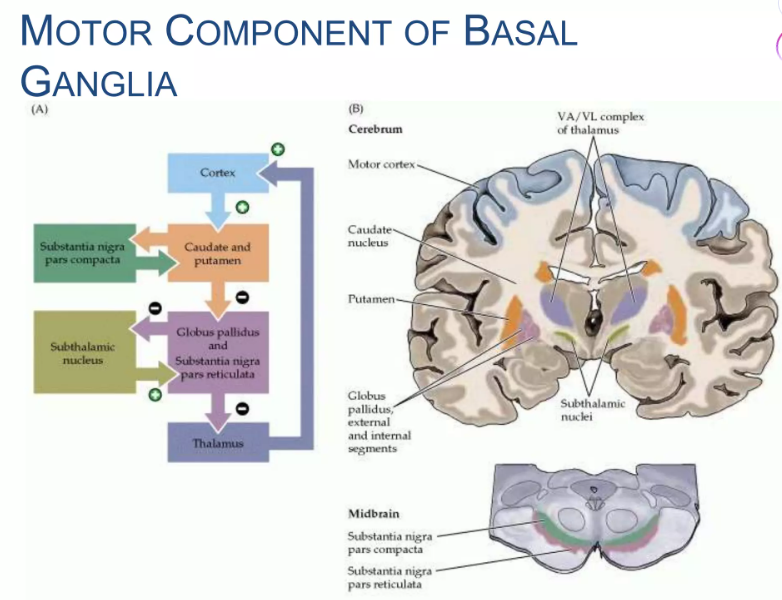
🔗 Major Connections and Circuits
- Cortico-striatal: Cortex → striatum (glutamate).
- Striato-pallidal/nigral: Striatum → GP/SNr (GABA).
- Pallido-thalamic: GPi/SNr → thalamus (GABA).
- Thalamo-cortical: Thalamus → motor cortex (glutamate).
Together, these form closed cortico–basal ganglia–thalamo–cortical loops, linking cortex back to itself.
➡️ Motor Pathways of the Basal Ganglia
✅ Direct Pathway (“GO” Pathway)
- Cortex → Striatum → GPi/SNr → Thalamus → Cortex.
- Striatum inhibits GPi/SNr.
- Reduced inhibition of thalamus.
- ↑ Thalamic excitation of cortex.
- → Facilitates movement.
⛔ Indirect Pathway (“STOP” Pathway)
- Cortex → Striatum → GPe → STN → GPi → Thalamus → Cortex.
- Activates STN → excites GPi.
- Increased thalamic inhibition.
- ↓ Cortical motor drive.
- → Suppresses unwanted movement.
🎭 Dopaminergic Modulation
- Dopamine from SNc modulates both pathways:
- D1 receptors: Stimulate direct pathway.
- D2 receptors: Inhibit indirect pathway.
- Net effect = promotion of movement.
Loss of dopamine removes both “acceleration” and “brake release”, producing excessive inhibition of the thalamus → bradykinesia and rigidity.
🔄 Functional Basal Ganglia Loops
- Motor loop: Motor cortex → putamen → GPi → thalamus → motor cortex.
- Associative loop: Prefrontal cortex → caudate → GP → thalamus → prefrontal cortex.
- Limbic loop: Limbic cortex → nucleus accumbens → ventral pallidum → thalamus → limbic cortex.
These parallel circuits explain why basal ganglia disease affects movement, cognition, and behaviour.
⚙️ Physiology of Basal Ganglia Function
- Action selection: Competing motor programmes are filtered; useful actions are facilitated, others suppressed.
- Scaling of movement: Regulates force, speed, and amplitude.
- Procedural learning: Dopamine signals reward prediction error → reinforces useful motor patterns.
- Timing and sequencing: Supports smooth chaining of movements.
- Automaticity: Converts conscious actions into habits (e.g. walking, typing).
Physiologically, the basal ganglia act as a dynamic gate between intention and execution, continuously adjusting motor output based on context and reward.
⚙️ Core Functions
- 🎯 Regulation of voluntary movement.
- 🔁 Habit formation and procedural memory.
- ❤️ Reward and motivation.
- 🧩 Executive and behavioural control.
- ⏱️ Motor timing and rhythm.
🏥 Clinical Relevance
- 🟤 Parkinson’s disease
- Loss of SNc dopamine neurons.
- ↓ Direct + ↑ Indirect pathway activity.
- Bradykinesia, rigidity, tremor, postural instability.
- 🔵 Huntington’s disease
- Degeneration of striatal GABA neurons.
- Reduced indirect pathway.
- Chorea, behavioural change, dementia.
- 🌀 Dystonia
- Abnormal basal ganglia output.
- Sustained muscle contractions and postures.
- 🤾 Hemiballismus
- STN lesion.
- Violent contralateral flinging movements.
- 🗣️ Tourette’s syndrome
- Disordered cortico–basal ganglia circuits.
- Motor and vocal tics.
📊 Key Structures and Functions
| Structure | Main Role | Pathway | Clinical Link |
|---|---|---|---|
| Striatum | Receives cortical input | Direct + Indirect | Huntington’s disease |
| GPi | Main output nucleus | Direct | Parkinsonian hypokinesia |
| GPe | Indirect modulation | Indirect | Dystonia |
| STN | Excites GPi | Indirect | Hemiballismus |
| SNc | Dopamine supply | Modulatory | Parkinson’s disease |
| Nucleus accumbens | Reward/motivation | Limbic | Addiction |
✅ Makindo Exam & Clinical Pearls
- Direct = GO, Indirect = STOP.
- Dopamine promotes movement via D1 and D2.
- Parkinson’s = too much thalamic inhibition.
- Huntington’s = too little thalamic inhibition.
- STN lesion = hemiballismus.
📌 Conclusion
The basal ganglia are specialised control centres that regulate movement, behaviour, and learning through interconnected cortico–thalamo–basal ganglia loops. By balancing direct and indirect pathways and modulating them with dopamine, they ensure that desired actions are facilitated while inappropriate ones are suppressed. Disruption of this finely tuned system produces characteristic neurological syndromes, making basal ganglia physiology central to understanding movement disorders.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery