
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Bacterial Meningitis in Children ✅
Related Subjects: |Acute Epiglottitis |Croup |Acute Tracheitis |Stridor |Acute Bacterial Meningitis in Children |Pneumonia in Children |Cystic Fibrosis |Sweat Test |Encopresis in Children |Enuresis/Bedwetting in Children |Acute Glomerulonephritis in Children |Nephrotic Syndrome in Children |Acute Appendicitis in Children |Gastro-oesophageal reflux in Children |Intussusception in Children |Panayiotopoulos Syndrome in Children |Reflex anoxic attacks in Children |Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections
🧠 Introduction
Meningococcal disease is a leading cause of bacterial meningitis and sepsis in children in the UK. It can progress rapidly and carries significant mortality and morbidity, including hearing loss, neurological impairment, and limb loss. Early recognition and immediate treatment are critical to survival.
| Paediatric Meningitis & Sepsis Pathway🚨 |
|---|
|
💉 Acute Bacterial Meningitis in Children
- A medical emergency involving infection of the meninges and often concurrent sepsis.
- Presentation may be non-specific early - do not wait for classical meningeal signs.
- Start IV antibiotics immediately - do not delay for lumbar puncture or imaging.
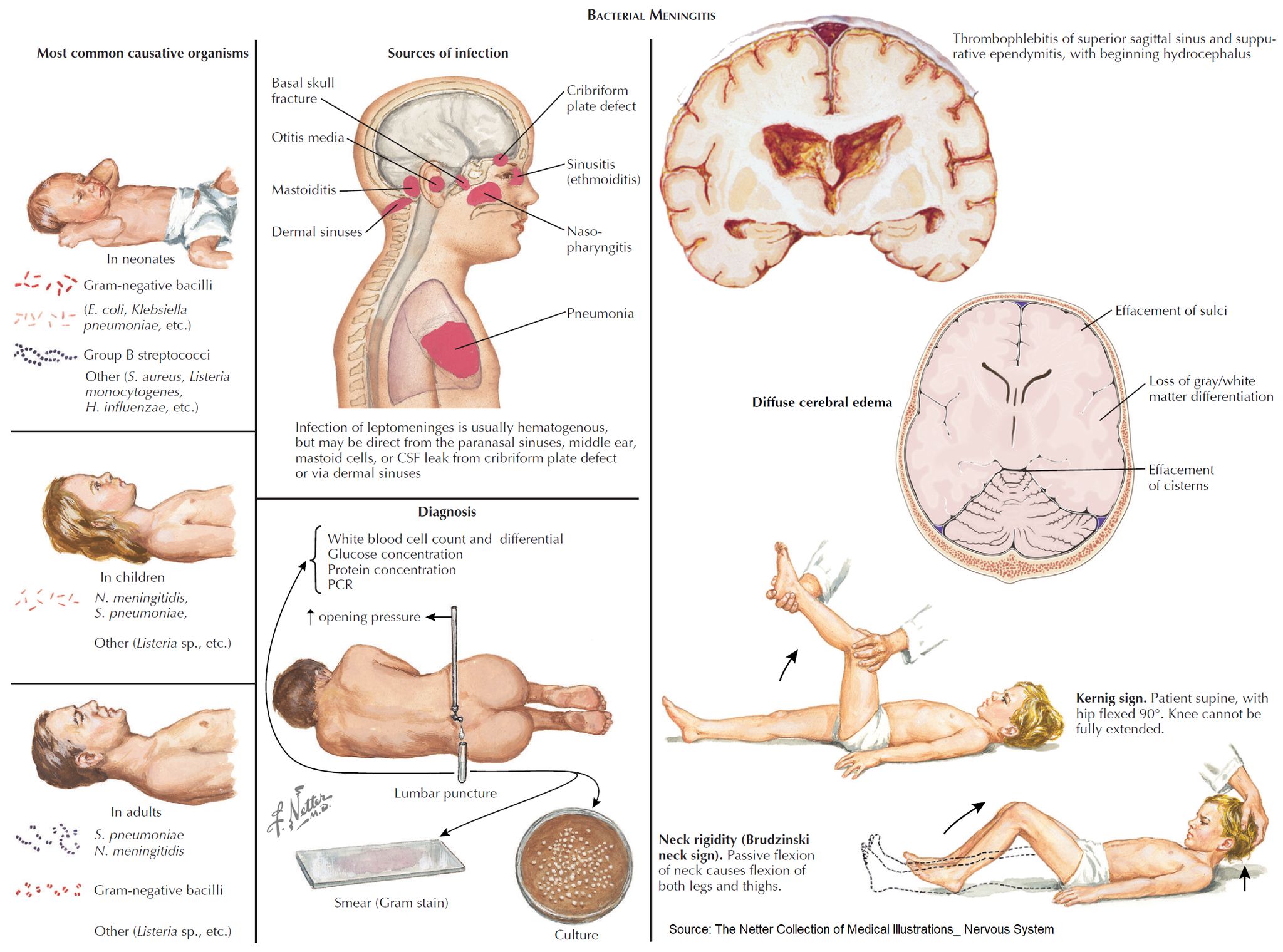
🦠 Common Causative Organisms (Age-Dependent)
- Neonates: Group B Streptococcus, Escherichia coli, Listeria monocytogenes.
- 1–3 months: Streptococcus pneumoniae, Neisseria meningitidis, GBS.
- >3 months: Neisseria meningitidis, Streptococcus pneumoniae.
- Haemophilus influenzae type b is now rare due to vaccination.
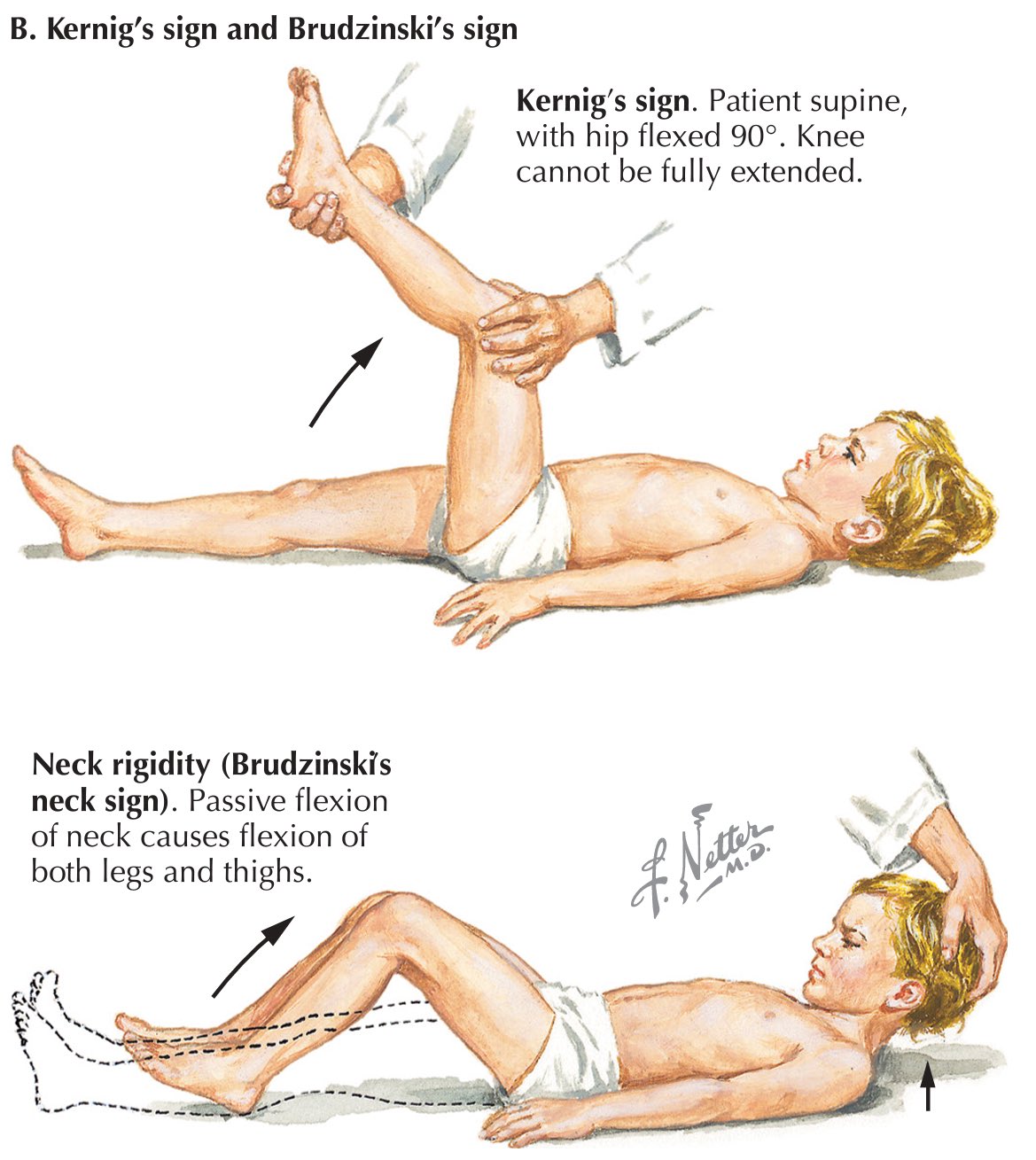
🚨 Red Flags (NICE Sepsis Features)
- Non-blanching rash (late sign).
- Altered consciousness or reduced responsiveness.
- Bulging fontanelle (infants).
- Neck stiffness, photophobia (often absent early).
- Limb pain, cold hands/feet, pale or mottled skin.
- Tachycardia, tachypnoea, hypotension (late).
- Seizures.
⚠️ Do not rely on rash or neck stiffness - early meningococcal disease often presents with fever, lethargy, and poor feeding. Think sepsis first in any unwell child.
🧪 Diagnosis
- Bloods: FBC, CRP, U&E, lactate, blood cultures (before antibiotics if no delay).
- PCR: for meningococcus/pneumococcus.
- Lumbar puncture: only if safe and will not delay treatment.
- Contraindications: shock, reduced GCS, focal neurology, papilloedema, coagulopathy.
- Imaging: not routine - only if signs of raised ICP or focal deficit.
💊 Pre-Hospital Antibiotics (UK NICE)
- Give IM benzylpenicillin if meningococcal disease suspected, unless it delays urgent transfer.
- Penicillin allergy → cefotaxime IM.
🏥 In-Hospital Management
🚨 Follow paediatric sepsis protocols: ABCDE, senior review, IV access, and antibiotics within 1 hour.
- <3 months: IV cefotaxime + amoxicillin (Listeria cover).
- >3 months: IV ceftriaxone (or cefotaxime).
- Add vancomycin if concern for resistant pneumococcus (local guidance).
💉 Adjunctive Treatment
- Dexamethasone: consider in suspected pneumococcal meningitis (give before or with first antibiotics).
- Fluids: cautious boluses (10–20 mL/kg) - reassess frequently (risk of cerebral oedema).
- Seizure control: benzodiazepines first-line.
- PICU referral: shock, respiratory failure, raised ICP.
🛡️ Prevention
- Vaccination: MenB, MenACWY, pneumococcal, Hib.
- Close contacts: give prophylaxis (e.g. rifampicin or ciprofloxacin) within 24 hours.
📈 Prognosis & Complications
- Mortality ~5–10% despite treatment.
- Complications: hearing loss, epilepsy, cognitive impairment, hydrocephalus, limb loss.
💡 Key Learning Point: In any unwell febrile child, treat for sepsis early and consider meningococcal disease. Delays in antibiotics are the biggest modifiable risk factor for death.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery