Cleft lip or palate
👶🧬 Cleft lip and/or palate is a common congenital craniofacial anomaly.
👨👩👧 If one first-degree relative in the family is affected, the recurrence risk for a child having a cleft lip and/or palate is approximately 2–5% - a small but important increase over the background population risk.
📘 About
- 📊 Incidence: approximately 16–17 per 10,000 live births in the UK.
- 👄 May present as cleft lip ± cleft palate.
- ⚖️ Can occur in isolation or as part of a genetic syndrome.
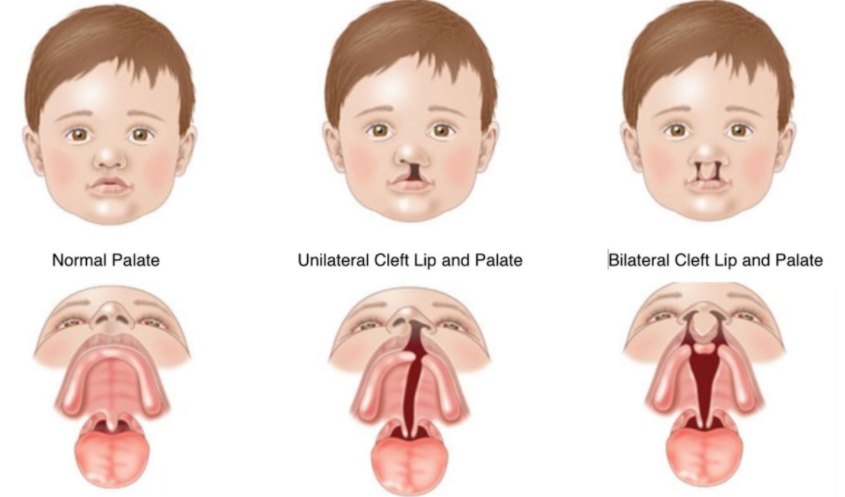
🧾 Classification / Description
- ➡️ Unilateral incomplete cleft lip
- ➡️ Unilateral complete cleft lip and palate
- ↔️ Bilateral complete cleft lip and palate
🧬 Aetiology & Embryology
- 🧠 The upper lip and palate form separately and at different gestational stages.
- ⏳ Cleft lip develops between weeks 4–6 of gestation (failure of fusion of the medial nasal and maxillary processes).
- ⏳ Cleft palate develops later, between weeks 6–12, due to failure of palatal shelf fusion.
- ⚠️ Lip and palate clefts often coexist, but arise from distinct embryological processes.
- 🧪 Multifactorial aetiology: genetic predisposition + environmental factors (e.g. maternal smoking, diabetes, folate deficiency).
🩺 Clinical Features
- 🍼 Feeding difficulty - poor latch, nasal regurgitation, prolonged feeds.
- 👀 Obvious facial cleft on inspection (lip).
- 👅 Always examine the oral cavity to assess palatal involvement.
- 📉 Risk of poor weight gain without early feeding support.
🧪 Investigations
- 🤰 Antenatal ultrasound may detect cleft lip.
- 🧠 Fetal MRI can detect cleft palate from around 15–16 weeks gestation.
- 👶 Diagnosis is confirmed on postnatal clinical examination.
- 🧬 Consider genetic assessment if syndromic features are present.
💊 Management
- 🍼 Feeding support is urgent:
- Specialist feeding assessment
- Special bottles or teats may be required
- ⚖️ Weekly weight monitoring initially
- 🏥 Early referral to the regional multidisciplinary cleft service:
- Cleft nurses
- Maxillofacial / plastic surgeons
- Speech & language therapists
- Audiology and ENT
- 🦷 Pre-surgical orthopaedics:
- Unilateral complete clefts → dentofacial maxillary appliance (DMA)
- Bilateral complete clefts → elastic chain premaxillary retraction (ECPR)
- Latham-type devices help approximate palatal segments before surgery
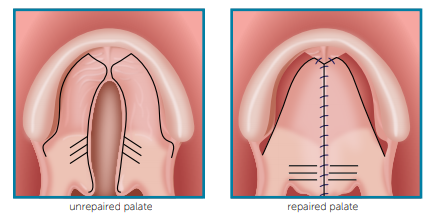
- ✂️ Surgical repair:
- 👄 Cleft lip repair at 3–5 months
(rotation-advancement, Millard, Mulliken techniques)
- 👅 Cleft palate repair at ~12 months
(two-flap palatoplasty or Furlow double-opposing Z-plasty)
- 👂 ENT complications:
- High risk of middle ear effusions
- Regular hearing surveillance
- Ventilation tubes (grommets) if persistent conductive hearing loss
🧠 Teaching & Exam Pearls
- ⚠️ Always inspect the palate in any baby with feeding difficulty.
- 🧬 Lip and palate clefts have different embryological timings.
- 🍼 Early feeding support prevents failure to thrive.
- 👂 OME and hearing loss are common - long-term follow-up is essential.
📚 References
- NHS Cleft Lip and Palate Service
- Royal College of Surgeons – Cleft Care Pathways
- NICE – Antenatal Screening & Congenital Anomalies
