
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anterior Spinal Cord syndrome
Related Subjects: | Transverse myelitis | Acute Disseminated Encephalomyelitis |Cervical spondylosis |Spinal Cord Anatomy |Acute Disc Prolapse |Spinal Cord Compression |Spinal Cord Haematoma |Foix-Alajouanine syndrome |Cauda Equina |Conus Medullaris syndrome |Anterior Spinal Cord syndrome |Central Spinal Cord syndrome |Brown-Sequard Spinal Cord syndrome
🧠 Anterior Spinal Cord Syndrome (ASCS) is an incomplete spinal cord injury involving the anterior two-thirds of the cord. It leads to motor paralysis and loss of pain/temperature sensation below the lesion, with sparing of vibration and proprioception (posterior columns). The commonest cause is anterior spinal artery infarction, but trauma and compression are also important. Prognosis is often poor compared to other incomplete cord syndromes.
📌 Introduction
- Spinal cord infarction is rare but catastrophic.
- 🩸 The anterior spinal artery supplies ~2/3 of the cord (motor + spinothalamic tracts) and is most vulnerable in the mid-thoracic "watershed" region (T4–T8).
- Injury here can arise from vascular, traumatic, or compressive causes.
⚠️ Causes
- Ischaemia: Aortic surgery, dissection, severe hypotension → anterior spinal artery occlusion.
- Trauma: Cervical/thoracic fracture–dislocation injuring anterior cord.
- Disc Herniation: Large central disc compressing anterior cord.
- Spinal Tumours: Neoplasms compressing blood supply.
- Infections: Spinal epidural abscess, transverse myelitis.
- Vascular Malformations: AVMs, aneurysms compromising flow.
🩻 Anatomy
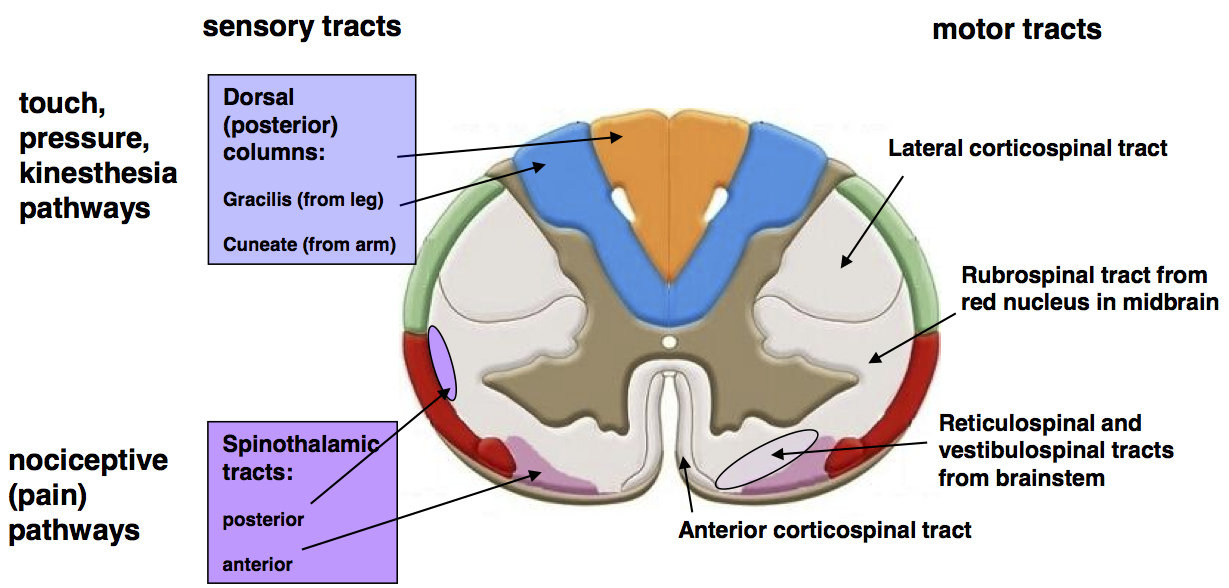
- Anterior spinal artery = single midline vessel running length of cord, reinforced by segmental arteries (e.g. artery of Adamkiewicz at T9–T12).
- Supplies corticospinal & spinothalamic tracts; posterior columns are spared (separate supply from posterior spinal arteries).
🧾 Clinical Features
- 💪 Motor: Paraplegia or quadriplegia (depending on level).
- 🔥 Pain/Temperature: Lost below lesion (spinothalamic tract).
- 🎯 Proprioception/Vibration: Preserved (dorsal columns spared).
- Bladder & bowel dysfunction common due to autonomic involvement.
- May present acutely (sudden vascular occlusion) or subacutely (compression/tumour).
🧠 Key Exam Pearl: “Anterior = motor & pain/temp loss, posterior = proprioception spared.”
🔍 Investigations
- MRI (gold standard): Identifies cord ischaemia, compression, tumours, or disc herniation.
- CT: Best for bony trauma, fractures, or dislocations.
- Spinal Angiography: Defines vascular occlusion/AVMs if intervention is planned.
🩺 Management
- 🔴 Acute: ABC resuscitation, spinal immobilisation (if trauma), maintain perfusion.
- 💊 Steroids: High-dose methylprednisolone is controversial; consider case-by-case.
- 🩸 Vascular: Endovascular repair, bypass, or stenting if vascular occlusion.
- 🔧 Surgical decompression: For cord compression (disc, tumour, haematoma).
- 🧑⚕️ Rehabilitation: Physiotherapy, occupational therapy, bowel/bladder management, DVT prophylaxis, and pressure sore prevention.
📊 Prognosis
- Recovery of motor function is usually poor, especially if initial paralysis is complete.
- Sensory sparing of proprioception often persists, aiding rehabilitation.
- Early diagnosis, decompression (if compressive), and optimisation of perfusion are key to improving outcomes.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery