
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Abdominal Pain in Adults
Related Subjects:Acute Cholecystitis |Acute Appendicitis |Chronic Peritonitis |Abdominal Aortic Aneurysm |Ectopic Pregnancy |Acute Cholangitis |Acute Abdominal Pain |Penetrating Abdominal Trauma |Abdominal Masses: Clinical Approach and Considerations |Abdominal Distension |Vomiting |Substance Misuse |Cannabinoid Hyperemesis Syndrome (CHS) |Cyclical Vomiting Syndrome
Acute abdominal pain accounts for ~5–10% of emergency department visits. Approximately 15–25% of cases require surgical intervention. The goal is rapid identification of surgical emergencies while avoiding unnecessary operations.
✅ Key Clinical Advice
- Always assess and stabilise with ABCDE before focusing on diagnosis.
- In unstable patients → urgent surgical review, do not delay for imaging.
- Consider broad differentials; elderly and immunosuppressed may have atypical presentations.
💊 Management
- 🔄 Resuscitation: ABCs, O₂, IV fluids, Fast patient NBM, catheter for urine output.
- 💉 Antibiotics: Broad-spectrum IV (e.g., Tazocin ± metronidazole).
- 💊 Analgesia: IV morphine (2.5–5 mg), antiemetics.
- 🧑⚕️ Urgent surgical referral: Early laparotomy/laparoscopy.
- 🧑⚕️Diagnostic triggers
- Abdominal pain + low BP → think sepsis
- Abdominal pain + low BP + >50 yrs → leaking AAA
- Abdominal pain + fertile female → ectopic pregnancy
- Abdominal pain + AF/MI → ischaemic bowel
- Abdominal pain + gallstones/alcohol → pancreatitis
🔪 Surgical Management
- Indicated for perforated viscus, bowel ischaemia, or generalised peritonitis.
- Procedures:
- Exploratory laparotomy/laparoscopy
- Resection of necrotic bowel, repair perforations
- Peritoneal lavage, drain abscesses
- Continue IV antibiotics post-op.
1. Initial Assessment & Red Flags
- ABCDE + vital signs + NEWS score
- Two large-bore IV access, bloods (FBC, U&E, CRP, lactate, amylase/lipase, LFTs, group & save ± crossmatch), urinalysis, pregnancy test (all women of childbearing age)
- Red flags requiring urgent senior/surgical input:
- Hypotension / tachycardia / shock
- Board-like rigid abdomen / generalised peritonism
- Pain out of proportion to examination findings
- Rising lactate (>2–4 mmol/L) or metabolic acidosis
- Free subdiaphragmatic air on erect CXR
- Elderly, diabetics, steroid/immunosuppressed patients (atypical / muted signs)
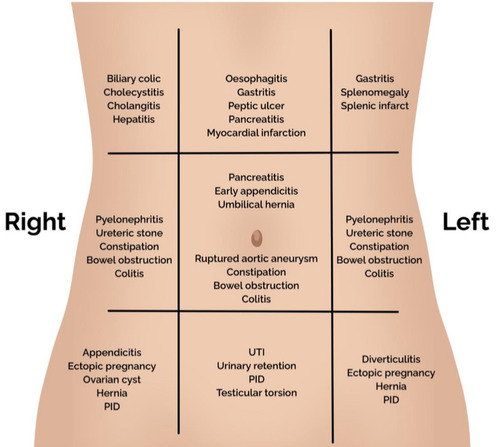
2. Differential Diagnosis by Anatomical Location
| Region | Common & Important Causes | Classic Clinical Features | First-line Investigations | Initial Management |
|---|---|---|---|---|
| Right Upper Quadrant (RUQ) | Acute cholecystitis
Cholangitis Biliary colic Perforated duodenal ulcer (referred) Hepatitis / liver abscess |
RUQ pain ± right shoulder tip
Murphy’s sign positive Charcot’s triad (fever + jaundice + RUQ pain) → cholangitis |
Abdominal ultrasound (first-line)
LFTs, FBC, CRP Blood cultures if febrile |
IV fluids, analgesia, IV antibiotics (if infection)
Early cholecystectomy (laparoscopic) for cholecystitis ERCP + antibiotics for cholangitis |
| Epigastric / Central | Perforated peptic ulcer
Acute pancreatitis Acute mesenteric ischaemia Aortic dissection / ruptured AAA Early appendicitis |
Sudden severe “knife-like” epigastric pain → perforation
Epigastric pain radiating to back → pancreatitis Severe pain out of proportion → ischaemia Tearing back/abdominal pain + shock → AAA |
Erect CXR (free air)
Amylase/lipase Lactate, CTA abdomen if ischaemia/AAA suspected Bedside US for AAA |
Resuscitation, NBM, IV PPI, broad-spectrum antibiotics, NG tube
Urgent laparotomy (perforation) Emergency vascular surgery (ruptured AAA) Heparin + revascularisation / resection (mesenteric ischaemia) |
| Right Lower Quadrant (RLQ) | Acute appendicitis
Mesenteric adenitis Ovarian torsion / ruptured cyst / ectopic Terminal ileitis (Crohn’s) |
Periumbilical → RLQ migration
Anorexia, nausea, low-grade fever Rebound / Rovsing’s sign |
FBC, CRP
Urine pregnancy test Ultrasound (young women / children) CT abdomen if diagnostic uncertainty |
IV fluids, analgesia, IV antibiotics
Laparoscopic appendicectomy |
| Left Lower Quadrant (LLQ) | Acute diverticulitis
Sigmoid volvulus Colonic perforation Ovarian / gynaecological pathology |
LLQ pain ± fever, change in bowel habit
Distension + tympany → volvulus |
CT abdomen/pelvis with IV contrast (gold standard)
AXR (coffee-bean sign in volvulus) |
IV fluids, IV antibiotics (e.g. co-amoxiclav or piperacillin-tazobactam)
Flexible sigmoidoscopy + decompression (volvulus without ischaemia) Surgery if perforation / peritonitis |
| Diffuse / Generalised | Generalised peritonitis (perforated viscus)
Bowel obstruction Mesenteric ischaemia Ruptured ectopic pregnancy Ruptured AAA |
Rigid “board-like” abdomen
Absent bowel sounds Shoulder tip pain (diaphragmatic irritation) |
Erect CXR (free air)
CT abdomen (most informative) β-hCG, FAST scan (ectopic) Bedside US or CTA (AAA / ischaemia) |
ABC resuscitation, broad-spectrum IV antibiotics, NBM, NG tube
Urgent laparotomy / laparoscopy |
3. Key Investigations – Tiered Approach
- Bedside / immediate: Pregnancy test, urinalysis, erect CXR (free air), ECG (exclude cardiac), FAST / POCUS (free fluid, AAA)
- Blood tests: FBC, U&E, CRP, lactate, amylase/lipase, LFTs, group & save / crossmatch, blood gas
- Imaging:
- Ultrasound: First-line for biliary, gynaecological, appendix (slim patients), AAA screening
- CT abdomen/pelvis with IV contrast: Gold standard for most acute surgical pathologies (perforation, ischaemia, diverticulitis, appendicitis in adults)
- CTA: Mesenteric ischaemia, aortic pathology
4. Antibiotic Choices (Empiric – Community-acquired)
- Mild–moderate: Co-amoxiclav IV or cefuroxime + metronidazole
- Severe / generalised peritonitis / healthcare-associated: Piperacillin-tazobactam (Tazocin) ± gentamicin (local policy)
- Cholangitis / biliary: Piperacillin-tazobactam or ceftriaxone + metronidazole
- Post-source control: Usually 4–5 days total; de-escalate / stop when clinically improved
5. Surgical vs Conservative Management Triggers
| Condition | Usually Surgical | Usually Conservative / Interventional |
|---|---|---|
| Appendicitis | Yes (laparoscopic appendicectomy) | Rarely antibiotics alone (selected uncomplicated cases) |
| Cholecystitis | Early laparoscopic cholecystectomy (within 7 days) | Antibiotics + percutaneous drainage (if unfit) |
| Perforated peptic ulcer | Yes (laparoscopic / open repair) | Very rare |
| Diverticulitis (uncomplicated) | No | IV antibiotics, fluids |
| Diverticulitis with abscess / perforation | Yes (often laparoscopic lavage or Hartmann’s) | Percutaneous drainage + antibiotics (selected cases) |
| Mesenteric ischaemia | Yes (revascularisation ± resection) | No |
| Ruptured AAA | Yes (open or EVAR) | No |
| Ruptured ectopic | Yes (salpingectomy / salpingostomy) | Methotrexate (stable, unruptured, selected cases) |
6. Final Key Take-home Messages
- Unstable or peritonism → theatre, not CT scanner
- Pregnancy test mandatory in women of reproductive age
- CT is the most useful single investigation in diagnostically uncertain cases in adults
- Pain out of proportion + atrial fibrillation / vascular risk → think acute mesenteric ischaemia
- Elderly / frail → assume surgical pathology until proven otherwise
- Early antibiotics + source control save lives in perforation / peritonitis
Always follow local protocols, consult senior clinicians, and refer to current trust / national guidelines (e.g., WSES 2024, NICE NG156, UpToDate 2026).
Case 1 – Perforated duodenal ulcer
A 48-year-old man with NSAID use develops sudden, severe epigastric pain radiating to the shoulder, rigid abdomen, and absent bowel sounds; vitals show tachycardia, low-grade fever, and mild hypotension. Erect CXR shows free subdiaphragmatic air. Manage with ABCDE, IV fluids, broad-spectrum antibiotics, PPI, NG tube, and urgent CT abdomen; refer for emergency surgery (laparoscopic Graham patch vs definitive ulcer surgery) and test/treat H. pylori after recovery.
Case 2 – Ruptured abdominal aortic aneurysm (AAA)
A 72-year-old man with smoking and hypertension presents with sudden tearing back/abdominal pain, hypotension, and a pulsatile abdominal mass. Avoid excessive fluids (permissive hypotension), give O₂, activate massive haemorrhage protocol, crossmatch, and call vascular surgery for immediate EVAR/open repair. POCUS/bedside ultrasound confirms large infrarenal AAA; do not delay for CT if unstable.
Case 3 – Ruptured ectopic pregnancy
A 30-year-old with 7 weeks’ amenorrhoea and vaginal spotting presents with worsening lower abdominal pain, dizziness, and shoulder tip pain; she is tachycardic and hypotensive with abdominal guarding. β-hCG positive; FAST scan shows free fluid. Resuscitate (O₂, IV access, bloods/crossmatch), consult gynae for urgent salpingectomy (or salpingostomy if appropriate), give anti-D if rhesus negative, and manage pain; differentials include ovarian torsion and ruptured corpus luteum.
Case 4 – Acute appendicitis
A 24-year-old develops periumbilical pain migrating to the RIF with anorexia, mild fever, and rebound tenderness; WBC/CRP raised. Ultrasound (slim female) or CT abdomen confirms inflamed, non-compressible appendix. Give IV fluids, analgesia, and broad-spectrum antibiotics; proceed to laparoscopic appendicectomy. Consider differentials (gynae, mesenteric adenitis); beware atypical retrocaecal pain.
Case 5 – Acute mesenteric ischaemia
A 78-year-old with AF has sudden, severe, diffuse abdominal pain out of proportion to scant early signs; lactate rising, metabolic acidosis. Urgent CTA shows SMA embolus. Resuscitate, start IV heparin and broad-spectrum antibiotics, involve vascular/HPB surgery for embolectomy/revascularisation ± bowel resection if non-viable; mortality is high-act fast.
Case 6 – Sigmoid volvulus
An 82-year-old in a care home presents with abdominal distension, pain, constipation, and tympany; X-ray shows the classic coffee-bean sign pointing to the RUQ. If no peritonitis/ischemia, perform flexible sigmoidoscopy with decompression and rectal tube; arrange definitive surgery (e.g., sigmoid colectomy) due to recurrence risk. If peritonitis or perforation, urgent laparotomy.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery