💥 Brachial neuritis, aka Parsonage-Turner syndrome or neuralgic amyotrophy, is an acute inflammatory disorder affecting the brachial plexus or its branches. It presents with sudden severe shoulder/upper arm pain, followed days to weeks later by patchy weakness, wasting and sensory symptoms. It may follow infection, vaccination, surgery, trauma, pregnancy, autoimmune disease or intense exertion, although many cases are idiopathic.
📖 About
- Inflammatory neuropathy of the brachial plexus or peripheral nerves around the shoulder girdle.
- May be post-infective or immune-mediated. Aetiology unclear.
- Usually unilateral, but may be bilateral.
- Recurrence is possible, especially in hereditary neuralgic amyotrophy.
🩺 Clinical Features
- ⚡ Severe acute shoulder, scapular or upper arm pain, often abrupt and worse at night.
- ➡️ Pain is followed by rapid-onset weakness and muscle wasting, often days to weeks later.
- Weakness is often patchy, not a single neat dermatome or myotome.
- Affects deltoid, supraspinatus, infraspinatus, serratus anterior and other plexus-supplied muscles.
- Scapular winging may occur if the long thoracic nerve is affected.
- 🤲 Sensory symptoms may occur, but motor weakness is often more prominent.
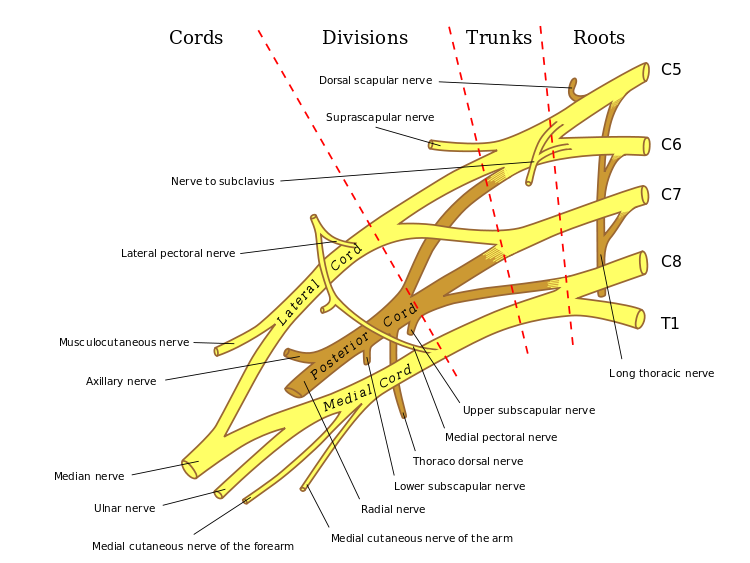
🧠 Anatomy: Brachial Plexus
🔍 Investigations
- Diagnosis is mainly clinical: severe acute pain followed by patchy weakness is the classic pattern.
- EMG / nerve conduction studies: can show denervation, localise affected nerves and support the diagnosis; most useful after 2-3 weeks.
- MRI cervical spine / brachial plexus / shoulder: if diagnostic uncertainty or to exclude radiculopathy, structural shoulder disease, tumour or other plexopathy.
- CXR / CT chest: consider if red flags for malignancy or compressive plexopathy, such as weight loss, cancer history, Horner syndrome, persistent progressive pain or suspicion of Pancoast tumour.
⚖️ Differentials
- Cervical radiculopathy - neck pain, dermatomal symptoms, reflex changes, pain affected by neck movement.
- Rotator cuff tear - mechanical shoulder pain and weakness, often related to injury.
- Frozen shoulder - restricted active and passive shoulder movement.
- Stroke/TIA - acute focal neurological deficit, face/speech/leg involvement or UMN signs.
- Traumatic or malignant plexopathy - progressive symptoms, cancer history, weight loss or severe persistent pain.
💊 Management
- Pain relief: NSAIDs/paracetamol if suitable; neuropathic pain agents such as amitriptyline, gabapentin, pregabalin or duloxetine may be needed.
- Severe early pain: short-course opioid analgesia may occasionally be required.
- Steroids: sometimes considered in the acute phase, but evidence is limited; discuss with neurology if severe or uncertain.
- Physiotherapy: maintain range of movement, prevent frozen shoulder, support scapular mechanics and gradually strengthen recovering muscles.
- Occupational therapy: consider for splints, work adaptations and functional support.
- Neurology referral: if severe weakness, diagnostic uncertainty, bilateral disease, respiratory symptoms, progressive deficit, recurrent episodes or poor recovery.
📈 Prognosis
- Pain often improves over weeks. Weakness may take months to years to recover.
- Many patients improve substantially, but residual weakness, fatigue, pain or wasting can persist.
🧠 Teaching point: The classic clue is the sequence: severe shoulder/arm pain first, then weakness later. Cervical radiculopathy usually follows a root pattern, while Parsonage-Turner syndrome is often patchy because it affects the brachial plexus or peripheral nerve branches.
