
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
OSCE Cranial nerves and examination
Related Subjects: |Cortical functions |Motor System |Sensory System |Mental state Examination |Speech and Language Exam |Cranial nerves and examination |Assessing Cognition
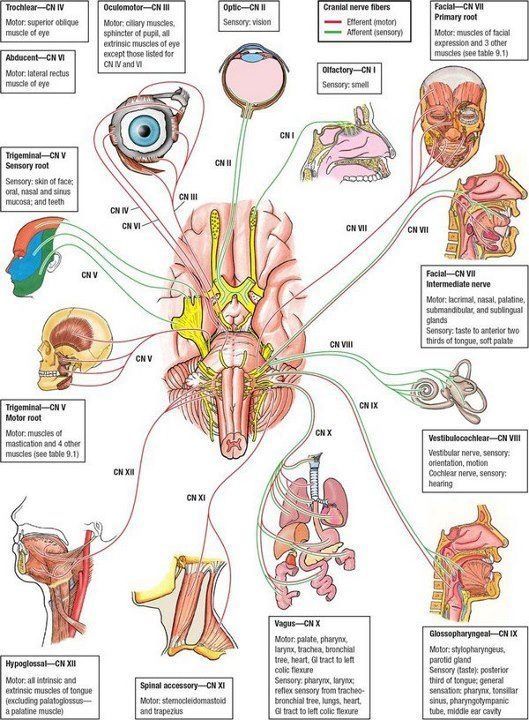
The Brainstem contains all the cranial nerves other than Olfactory and optic nerves
🧠 Brainstem Anatomy & Cranial Nerves
💡 The brainstem contains the nuclei of most cranial nerves (III–XII). Cranial nerves I and II are not true brainstem nerves: they arise from the forebrain. A helpful rule is: midbrain = III, IV; pons = V, VI, VII, VIII; medulla = IX, X, XI, XII.
| Nerve | Main nucleus location | Main branches / divisions | Key anatomy & function |
|---|---|---|---|
| I. Olfactory 👃 | Above brainstem | No major named branches | Special sensory nerve for smell. Fibres pass through the cribriform plate to the olfactory bulbs and tracts. Not a true peripheral nerve in the same way as the others. |
| II. Optic 👁️ | Above brainstem; synapses in the lateral geniculate nucleus of the thalamus | No major named branches | Special sensory nerve for vision. Arises from retinal ganglion cells, passes through the optic canal, partially decussates at the optic chiasm, then continues as the optic tract. |
| III. Oculomotor 👁️🗨️ | Midbrain at the level of the superior colliculus | Superior and inferior divisions in the orbit | Motor to SR, IR, MR, IO and levator palpebrae superioris. Parasympathetic fibres from the Edinger–Westphal nucleus constrict the pupil and accommodate the lens. Exits the midbrain between the PCA and SCA; vulnerable to posterior communicating artery aneurysm. |
| IV. Trochlear 🔄 | Midbrain at the level of the inferior colliculus | No major named branches | Motor to superior oblique. The only cranial nerve to exit dorsally from the brainstem and the only one to cross completely before exiting, so each nucleus supplies the contralateral muscle. |
| V. Trigeminal 😬 | Pons; with sensory nuclei extending into midbrain and medulla |
|
Main sensory nerve of the face and motor nerve to the muscles of mastication. Large sensory and smaller motor roots emerge from the lateral pons. V1 and V2 are sensory only; V3 is mixed. |
| VI. Abducens ↔️ | Pons (abducens nucleus in the dorsal pons) | No major named branches | Motor to lateral rectus, which abducts the eye. Emerges at the pontomedullary junction, travels through the cavernous sinus, and enters the orbit via the superior orbital fissure. Vulnerable in raised ICP because of its long intracranial course. |
| VII. Facial 🙂 | Pons |
|
Motor to facial expression, taste to the anterior two-thirds of the tongue, parasympathetic to lacrimal and submandibular/sublingual glands, and a small sensory component to the ear. Fibres loop around the abducens nucleus, forming the facial colliculus. |
| VIII. Vestibulocochlear 🎧 | Pons / pontomedullary junction |
|
Special sensory nerve for hearing and balance. Enters the internal acoustic meatus with VII. Lesions may cause hearing loss, vertigo, nystagmus, and imbalance. |
| IX. Glossopharyngeal 👅 | Medulla | No major named branches usually emphasized in basic anatomy | Taste and sensation from the posterior one-third of the tongue, sensory limb of the gag reflex, stylopharyngeus motor supply, and parasympathetic supply to the parotid gland. |
| X. Vagus 🫁 | Medulla |
|
Motor to the palate, pharynx, and larynx; parasympathetic supply to thoracic and abdominal viscera; sensory from larynx and viscera. Important for voice, swallowing, and autonomic control. |
| XI. Accessory 💪 | Spinal accessory nucleus in the upper cervical cord; cranial root from medulla | No major named branches | Motor to sternocleidomastoid and trapezius. Responsible for head turning and shoulder shrug. |
| XII. Hypoglossal 👄 | Medulla | No major named branches | Motor to the intrinsic and extrinsic muscles of the tongue (except palatoglossus). Emerges between the pyramid and olive. Lesions cause tongue weakness and deviation. |
🖼️ Image
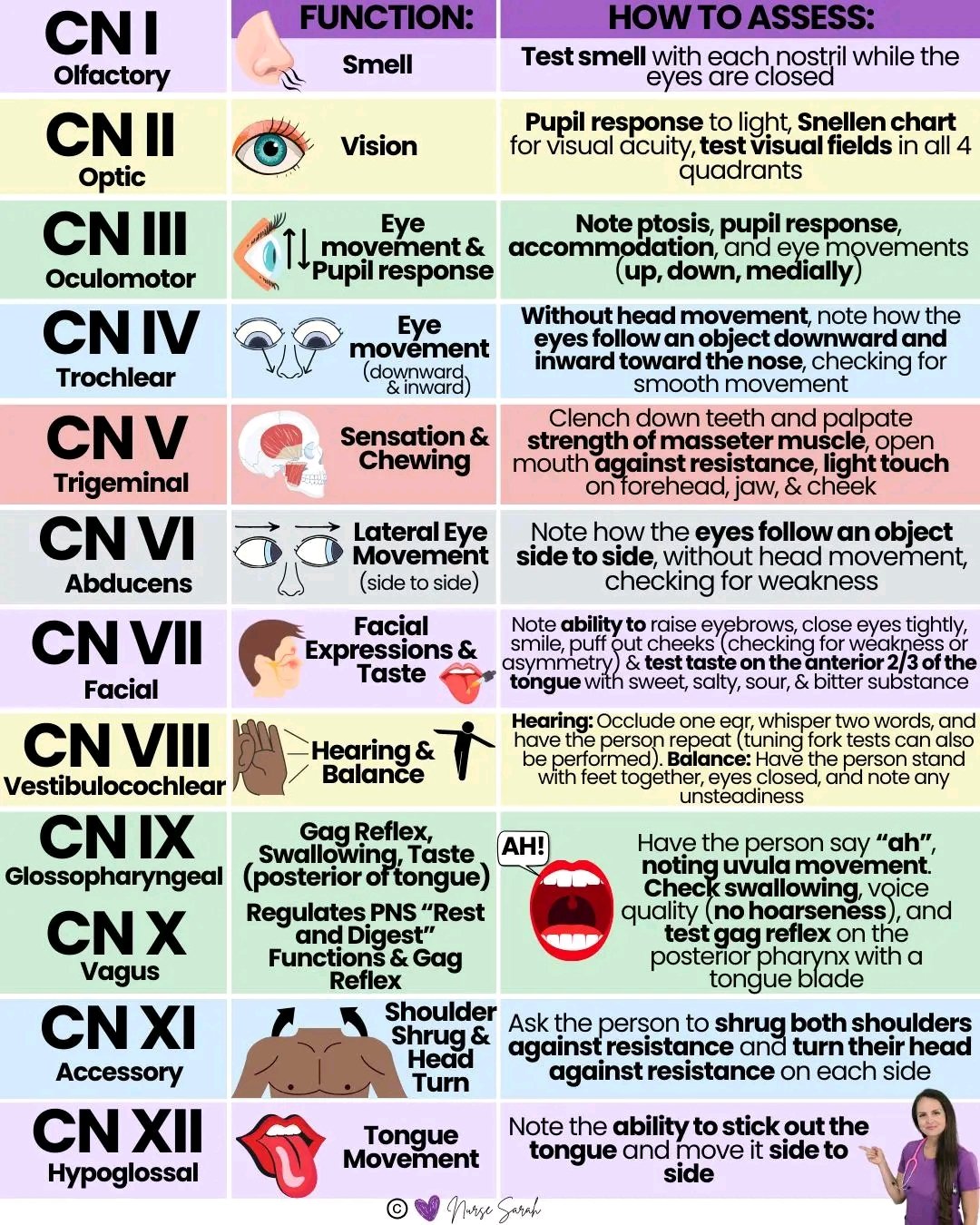
🩺 Examination of Cranial Nerves
🎯 In OSCEs, cranial nerve examination is really about linking function to anatomy. Always observe first: look for ptosis, facial asymmetry, nystagmus, dysarthria, tongue wasting, and abnormal eye position before you start formal testing.
| Cranial nerve | Name | How to examine |
|---|---|---|
| I | 👃 Olfactory | Test each nostril separately with a familiar non-irritant smell such as coffee or vanilla. Rarely tested routinely unless clinically relevant. |
| II | 👁️ Optic | Assess visual acuity, visual fields by confrontation, and inspect the pupils for direct and consensual light responses. Fundoscopy may be added. |
| III | 👁️🗨️ Oculomotor | Look for ptosis, pupil size, and eye position. Test eye movements, especially up, down, and in. Assess light reflex and accommodation. |
| IV | 🔄 Trochlear | Test downward and inward movement of the eye. Ask about vertical diplopia, especially when looking down (e.g. walking downstairs). |
| V | 😬 Trigeminal | Test facial sensation in the V1, V2, and V3 territories. Palpate the masseter and temporalis as the patient clenches their teeth. Corneal reflex may be tested if relevant. |
| VI | ↔️ Abducens | Assess abduction of the eye by asking the patient to follow your finger laterally. Failure suggests lateral rectus weakness. |
| VII | 🙂 Facial | Ask the patient to raise eyebrows, close eyes tightly, show teeth, smile, and puff out cheeks. Check for asymmetry and distinguish UMN from LMN weakness. |
| VIII | 🎧 Vestibulocochlear | Assess hearing with whispered voice or finger rub, then use Rinne and Weber tests if needed. Ask about vertigo, tinnitus, and balance problems. |
| IX | 👅 Glossopharyngeal | Assess swallowing history and gag reflex if needed. Sensory limb of gag reflex is mainly IX. In practice, IX and X are usually tested together. |
| X | 🫁 Vagus | Listen for hoarseness. Ask the patient to say “ah” and inspect palatal movement and uvular position. Ask about swallowing and coughing. |
| XI | 💪 Accessory | Test trapezius by shoulder shrug against resistance and sternocleidomastoid by head turn against resistance. |
| XII | 👄 Hypoglossal | Ask the patient to protrude the tongue and move it side to side. Look for deviation, wasting, or fasciculations. |
🧠 Quick localisation tip:
III–IV = midbrain
V–VIII = pons
IX–XII = medulla / upper cervical region
💡 A lesion in the brainstem often gives an “alternating” pattern: ipsilateral cranial nerve signs with contralateral limb weakness or sensory loss.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery