Related Subjects:
|Initial Trauma Assessment and Management
|Thoracic Trauma Assessment and Management
|Flail Chest Rib fractures
|Resuscitative Thoracotomy
|Haemorrhage control
|Traumatic Head/Brain Injury
|Traumatic Cardiac Arrest
|Abdominal trauma
|Tranexamic Acid
|Silver Trauma
|Cauda Equina
|Rib Fracture Score
Introduction
- 💥 Traumatic rib fractures are common after blunt chest trauma, with significant morbidity and mortality.
- 🫁 Respiratory complications (esp. pneumonia) occur in up to 31% of cases → early recognition and aggressive pain management are vital.
- 💊 Multimodal analgesia prevents hypoventilation and secretion retention, combining systemic + regional techniques.
- 🔧 In selected patients, surgical fixation improves outcomes by stabilising the chest wall.
Risk Factors
- 👴 More common in elderly due to osteoporosis and frailty.
- 🚗 High-energy trauma (RTAs, falls from height, crush injuries).
- 🦴 Underlying bone disease (osteoporosis, metastatic disease, myeloma).
Epidemiology
- 📊 Rib fractures in ~10% of all trauma patients.
- ~75% from blunt thoracic trauma, esp. RTAs.
- Associated with significant morbidity; severe cases → mortality up to 33%.
Pathophysiology
- 😣 Hypoventilation due to pain → atelectasis, impaired clearance, pneumonia.
- 🫀 Impaired gas exchange → pulmonary contusions, intrapulmonary shunting, hypoxia.
- 🫁 Altered mechanics → flail chest causes paradoxical movement, ↑ work of breathing, ↓ tidal volume.
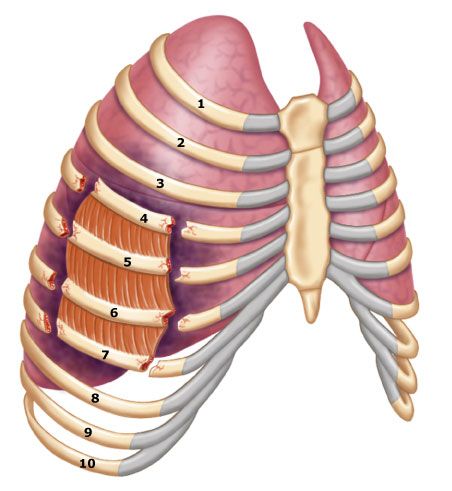
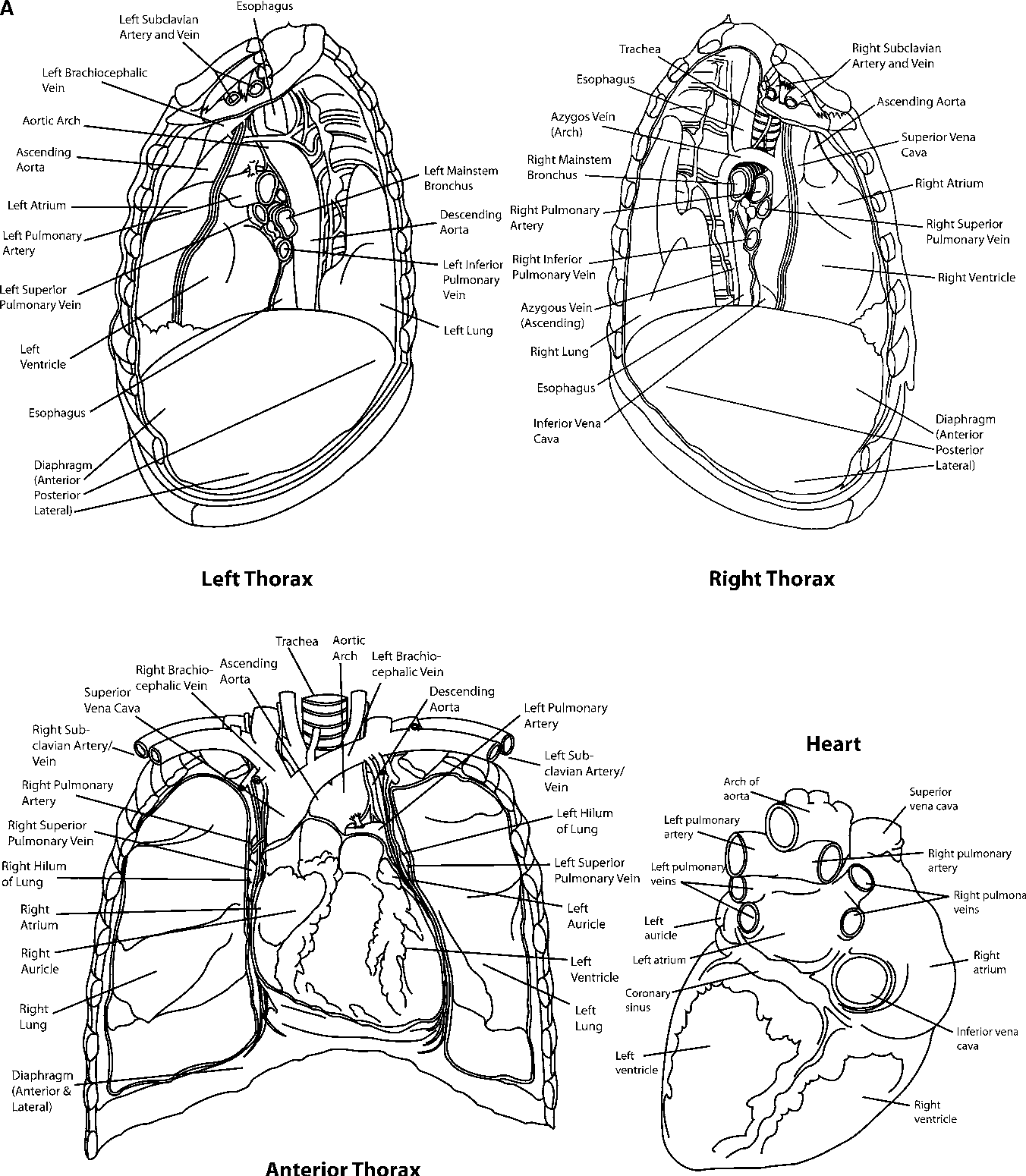
Associated Injuries
- 1st/2nd rib → subclavian vessels, aorta, trachea, bronchus.
- Sternum → myocardium, great vessels, thoracic spine.
- Lower ribs → right = liver/kidney, left = spleen/kidney.
Flail Chest
- Multiple adjacent ribs fractured in ≥2 places → segment moves paradoxically.
- Paradoxical breathing worsens hypoxia, esp. with lung contusion.
Myocardial Contusion
- Often with sternal fractures.
- Features: chest pain, tachycardia, raised JVP, arrhythmias, troponin rise.
- ECG: arrhythmia, BBB, ST changes.
- Management: CCU/HDU monitoring, echocardiography if significant.
🔎 Investigations
- 🧪 Bloods: FBC, U&E, LFTs, Amylase, Lactate, ABG.
- ❤️ Cardiac markers: CK, Troponin.
- 🩻 Imaging: CXR, CT Traumogram (gold standard for extent & associated injuries).
Management & Rib Fracture Score (RFS)
- 🔑 ABC first → oxygen to maintain SpO₂ 94–98% (unless COPD).
- 💊 Pain control ladder:
- Paracetamol 1 g PO/IV q6h
- Ibuprofen 400 mg q8h (with PPI)
- Lidocaine 5% plaster
- Morphine PO/PRN or MST regularly
- Adjuncts e.g. Gabapentin for neuropathic pain
- 🧾 RFS thresholds:
- RFS ≤ 5 → ward care, oral/IV analgesia
- RFS 6–10 → PCA, consider regional block, HDU
- RFS ≥ 10 → ICU, thoracic epidural / paravertebral block
- 🏃 Early physiotherapy, incentive spirometry, mobilisation to reduce pneumonia risk.
Surgical Repair of Flail Chest
- Indicated in severe flail chest, respiratory failure, or prolonged ventilation.
- Fixation improves chest wall mechanics, ↓ pain, ↓ ICU stay, ↓ pneumonia risk.
Epidurals & Regional Analgesia
- Best for multiple/bilateral fractures, flail segments, severe pain.
- Contraindications:
- Absolute: spinal injury, coagulopathy, local infection, patient refusal.
- Relative: anticoagulation, spinal fractures, ↑ICP.
- Complications: Hypotension, motor block, urinary retention, opioid-related pruritus.
Complications & Prevention
- 🫁 Pneumonia – prevented by pain control, chest physio, mobilisation.
- 💔 Arrhythmias – screen for cardiac contusion in sternal fractures.
- 🩸 VTE – prophylaxis with LMWH unless contraindicated.
- 🧠 Delirium (elderly) – optimise pain, sleep, minimise opioids where possible.
🌟 Clinical Pearl: Pain control = the single most important intervention. Poor analgesia → hypoventilation → pneumonia → ICU admission.
References
