Neuroscience - Vision and Eye movements
The 6 extraocular muscles in each eye precisely position the globe so that light falls on the fovea, the area of highest visual acuity.
👀 Coordinated conjugate eye movements keep both eyes aligned on the same target, allowing binocular single vision.
💡 Disruption of this system causes diplopia, strabismus, or impaired gaze control.
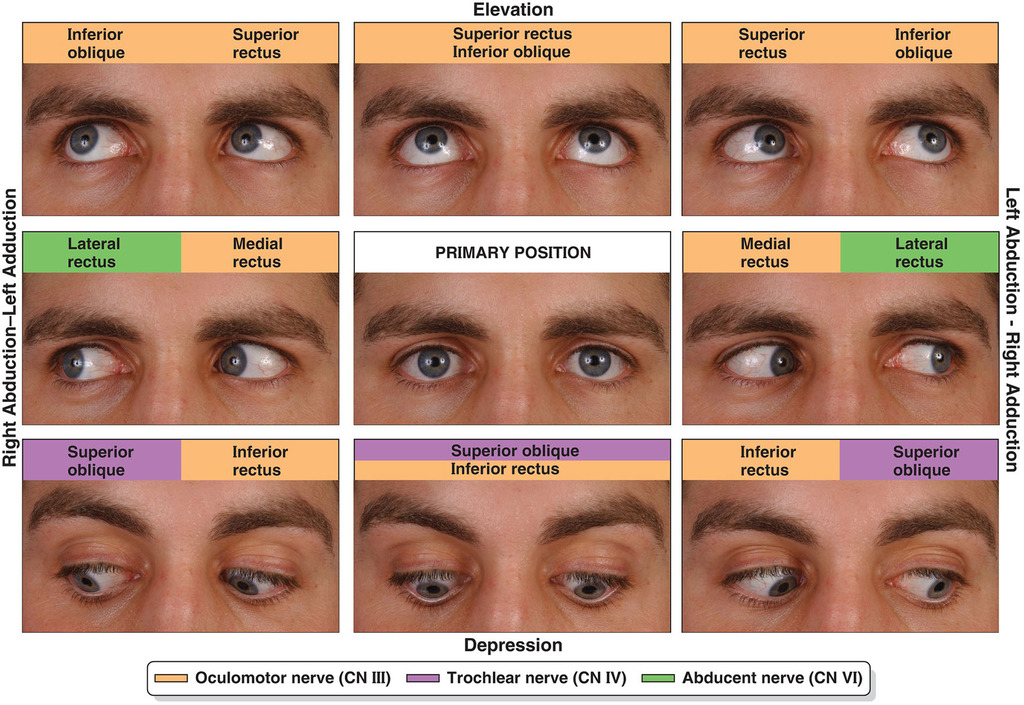
- 🧠 Extraocular Muscles & Innervation
- Lateral rectus: abducts eye → CN VI (abducens)
- Medial rectus: adducts eye → CN III (oculomotor)
- Superior rectus: elevates, adducts, intorts → CN III
- Inferior rectus: depresses, adducts, extorts → CN III
- Superior oblique: depresses, abducts, intorts → CN IV (trochlear)
- Inferior oblique: elevates, abducts, extorts → CN III

🎯 Principal Types of Eye Movements
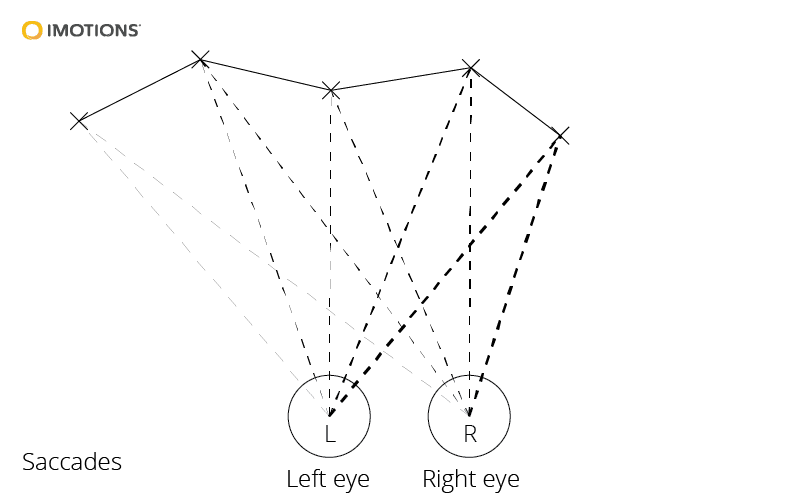
- ⚡ Saccades: rapid, ballistic eye movements that shift fixation from one target to another, such as during reading or scanning a room.
Generated mainly by the frontal eye fields, parietal eye fields, and superior colliculus, with burst neurons in the PPRF for horizontal movements and riMLF for vertical movements.
- 🎥 Smooth pursuit: slow, continuous tracking of a moving target.
Requires cortical motion areas such as MT/MST, cerebellar modulation, and brainstem gaze pathways.
- 🌀 Vestibulo-ocular reflex (VOR): stabilises gaze during head movement by moving the eyes in the opposite direction to head rotation.
Driven by the semicircular canals → vestibular nuclei → ocular motor nuclei.
💡 This is why you can keep your eyes on a target while your head moves.
- 🔍 Vergence / convergence: disconjugate movements that align both eyes for near vision.
Part of the near triad: convergence + accommodation + miosis.
⚠️ Strabismus & Diplopia
- Strabismus = misalignment of the visual axes.
- Diplopia occurs when the eyes are misaligned and both foveae are no longer directed at the same target.
- Common causes include:
- 🧠 CN III, IV, or VI palsies
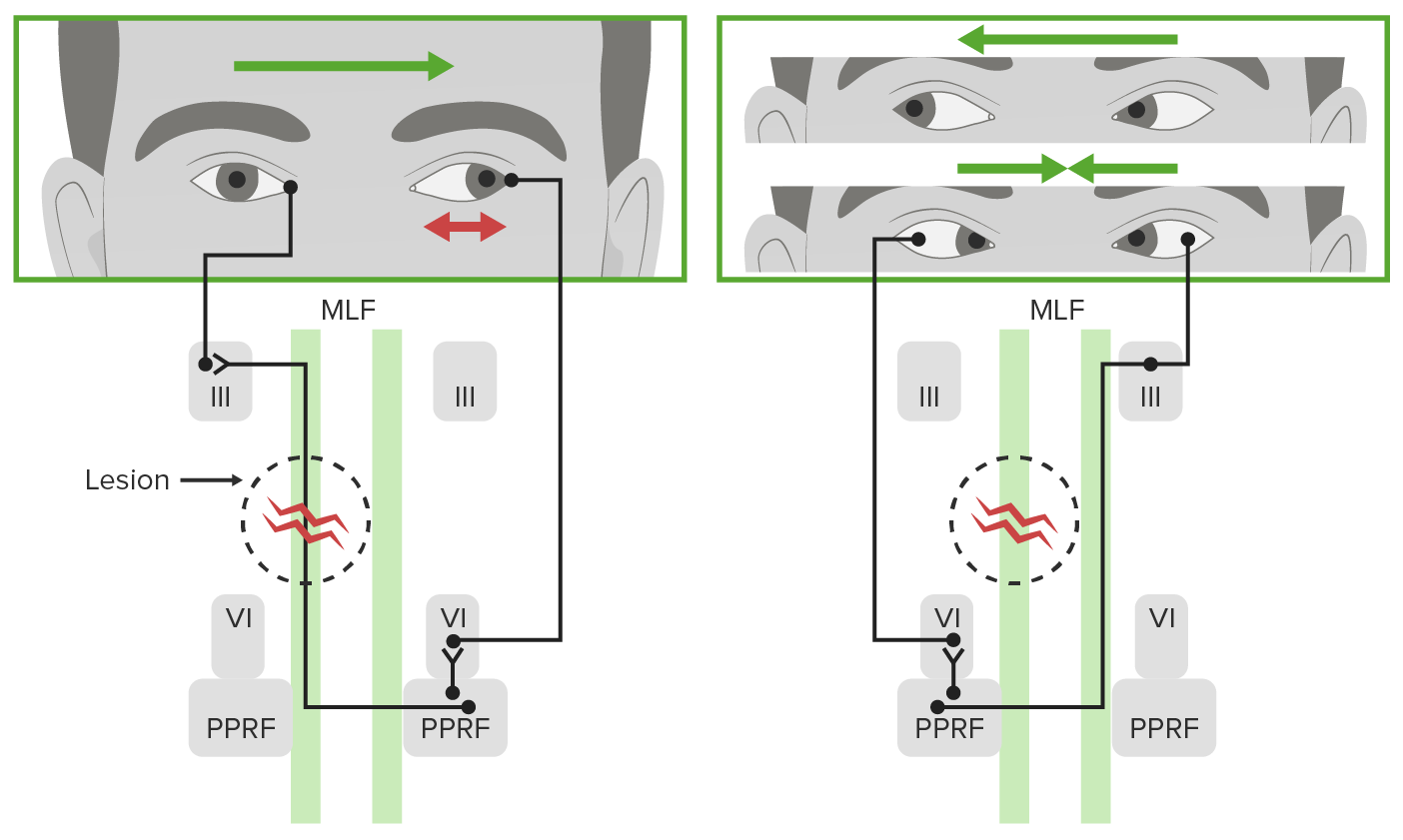
- 🔗 Internuclear ophthalmoplegia (INO) due to MLF lesion
- 💪 Myasthenia gravis
- 🦋 Thyroid eye disease
- 🚨 Brainstem stroke
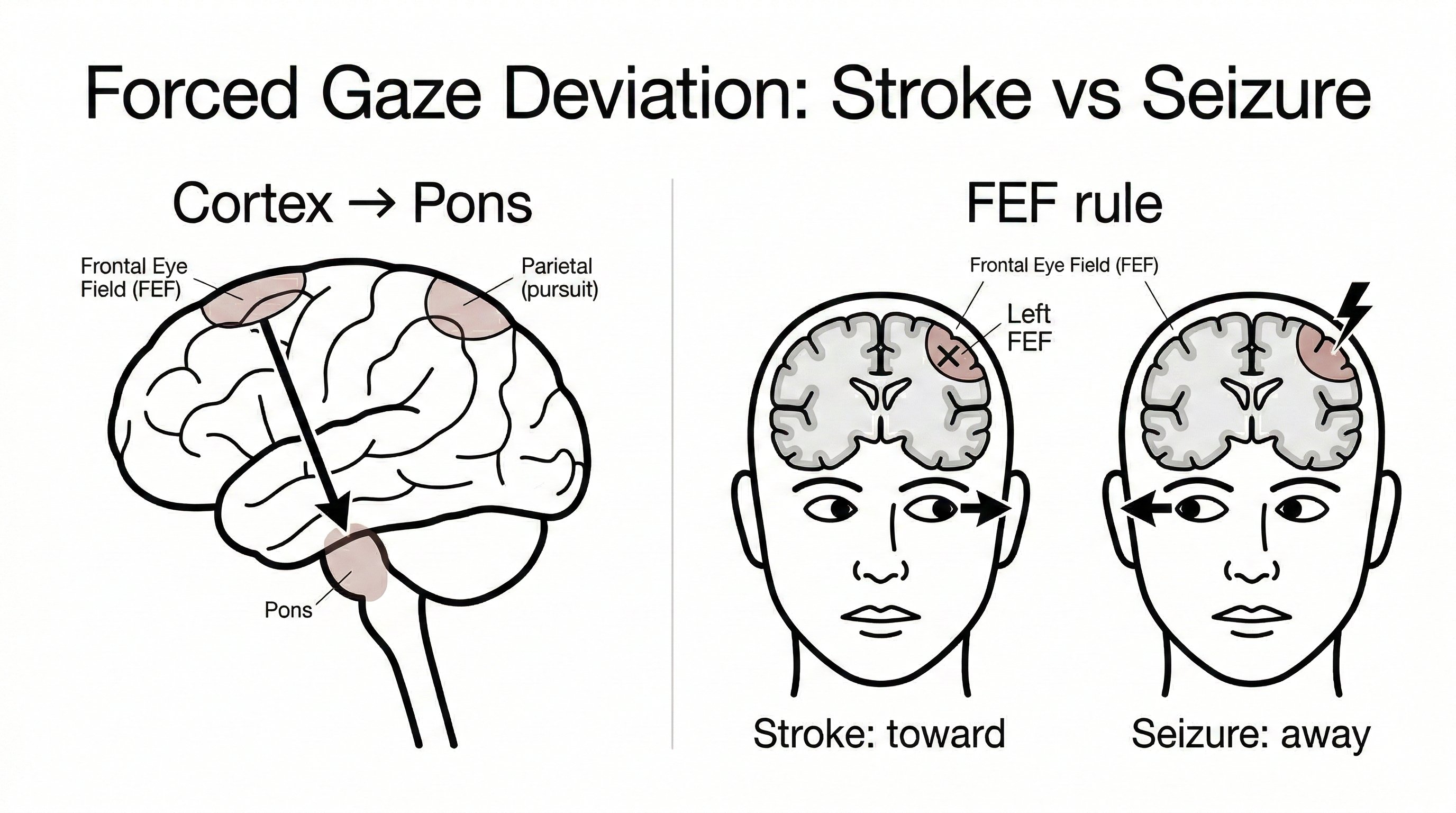
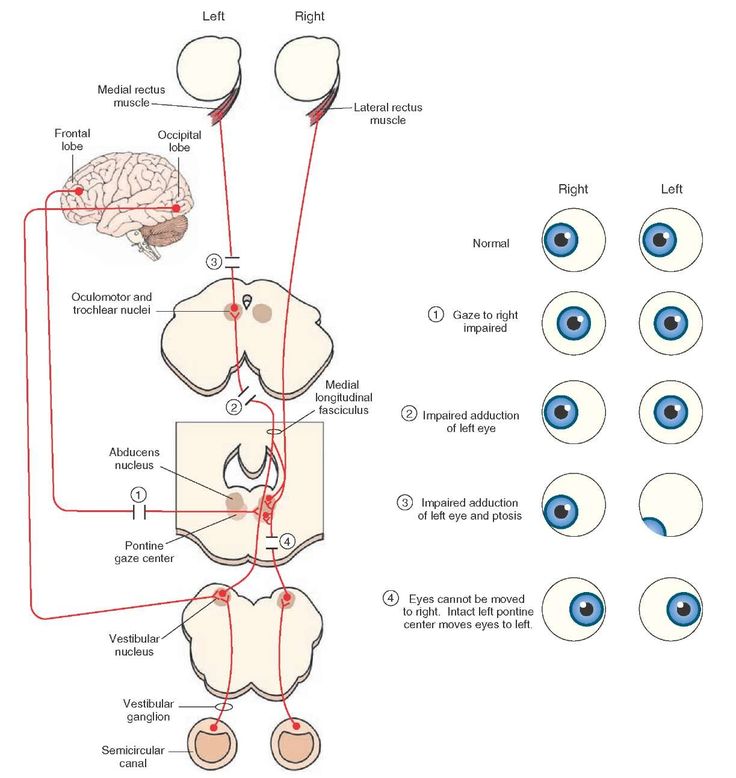
↔️ Horizontal Gaze Control
- 🧩 Key Structures
- PPRF (paramedian pontine reticular formation): horizontal saccade generator
- Abducens (VI) nucleus: contains:
- motor neurons to the ipsilateral lateral rectus
- internuclear neurons projecting via the MLF to the contralateral III nucleus for medial rectus activation
- MLF (medial longitudinal fasciculus): coordinates conjugate horizontal gaze
- Vestibular nuclei: integrate head-movement signals into eye movements
- ➡️ Mechanism of rightward gaze
- The right PPRF activates the right VI nucleus.
- This causes:
- right lateral rectus contraction
- signal via the left MLF to the left III nucleus → left medial rectus contraction
- The result is conjugate gaze to the right.
- 🚨 Classic lesion patterns
- PPRF lesion → ipsilateral gaze palsy
- MLF lesion → INO: impaired adduction of the affected eye with abducting nystagmus of the opposite eye
- Abducens nucleus lesion → ipsilateral horizontal gaze palsy
↕️ Vertical Gaze Control
- Vertical gaze centres are located mainly in the rostral midbrain.
- riMLF (rostral interstitial nucleus of the MLF) generates vertical saccades.
- Interstitial nucleus of Cajal helps maintain vertical gaze position.
- These pathways coordinate:
- CN III → superior and inferior recti, inferior oblique
- CN IV → superior oblique
- 🚨 Dorsal midbrain (Parinaud) syndrome classically causes:
- upgaze palsy
- convergence-retraction nystagmus
- light-near dissociation
👓 Binocular Vision
- Binocular single vision requires accurate alignment of both eyes on the same target.
- This depends on:
- PPRF + abducens nucleus for horizontal gaze
- Midbrain convergence centres for near gaze
- MLF for internuclear coordination
- Vestibular inputs to stabilise gaze during head movement
- Example: if the head turns suddenly to the right, the vestibular system generates compensatory leftward eye movement to keep vision stable.
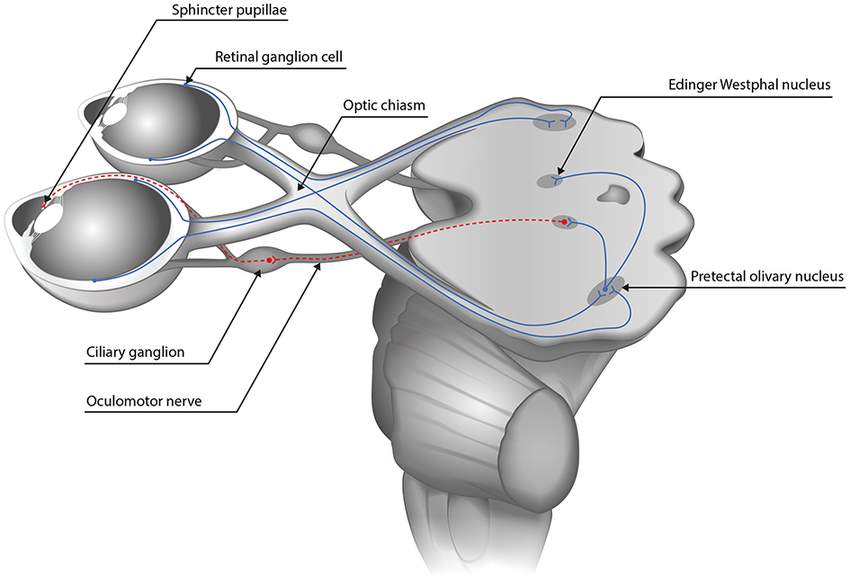
👁️🗨️ Pupils
- 🔹 Miosis (constriction): parasympathetic pathway
- Edinger–Westphal nucleus → CN III → ciliary ganglion → short ciliary nerves → sphincter pupillae
- 🔸 Mydriasis (dilation): sympathetic pathway
- Hypothalamus → ciliospinal centre (C8–T2) → superior cervical ganglion → long ciliary nerves → dilator pupillae
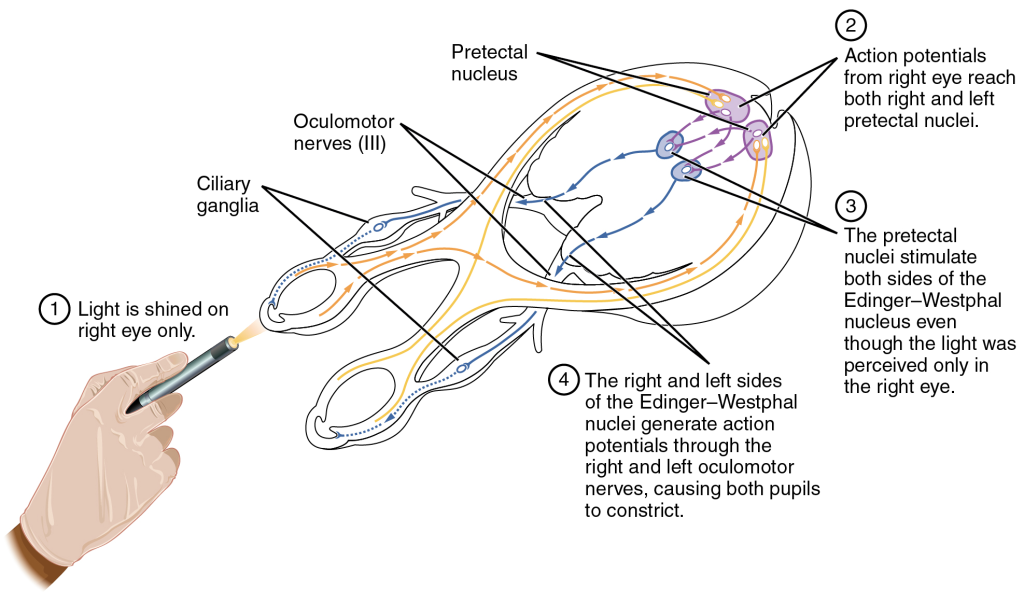
- 💡 Light reflex
- Afferent limb: CN II
- Signal passes to the pretectal nuclei
- Then bilaterally to the Edinger–Westphal nuclei
- This produces both:
- direct light reflex
- consensual light reflex
- RAPD (Marcus Gunn pupil) indicates an afferent pathway defect.
- 📚 Accommodation reflex (near triad)
- Convergence of both eyes
- Lens accommodation via ciliary muscle
- Miosis
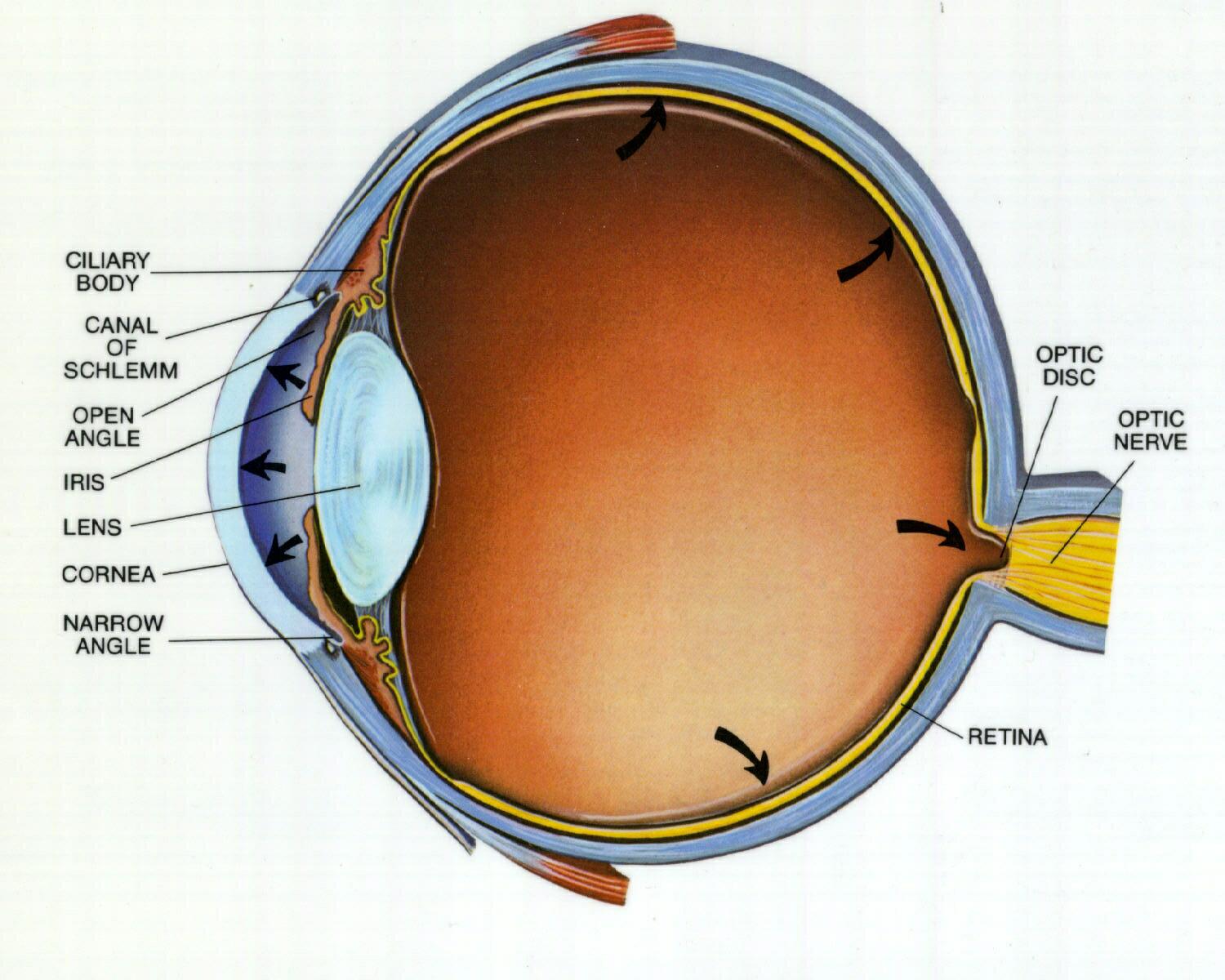
🧠 Retina
- Light passes through the inner retinal layers before reaching the photoreceptors (rods and cones).
- Unlike most neurons, photoreceptors hyperpolarise in response to light, reducing glutamate release.
- This signal is then processed through:
- bipolar cells
- ganglion cells - the first cells in the visual pathway to generate action potentials
- Horizontal cells and amacrine cells provide lateral modulation, improving contrast and visual processing.
- 🎯 Fovea:
- cone-rich
- avascular
- thin inner layers
- site of highest visual acuity and colour vision
- ⚫ Optic disc:
- site where ganglion cell axons leave the eye
- contains no photoreceptors
- creates the physiological blind spot

💡 Key summary:
👁️ Eye movements depend on the precise coordination of CN III, IV, and VI, brainstem gaze centres, the MLF, and vestibular input.
↔️ Horizontal gaze is organised through the PPRF–VI nucleus–MLF–III nucleus pathway.
↕️ Vertical gaze depends mainly on the rostral midbrain.
👁️🗨️ Pupil reflexes test both afferent (CN II) and efferent parasympathetic (CN III) pathways.
🧠 The retina is not just a camera sensor - it is active neural tissue that performs early visual processing before signals even leave the eye.
