
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
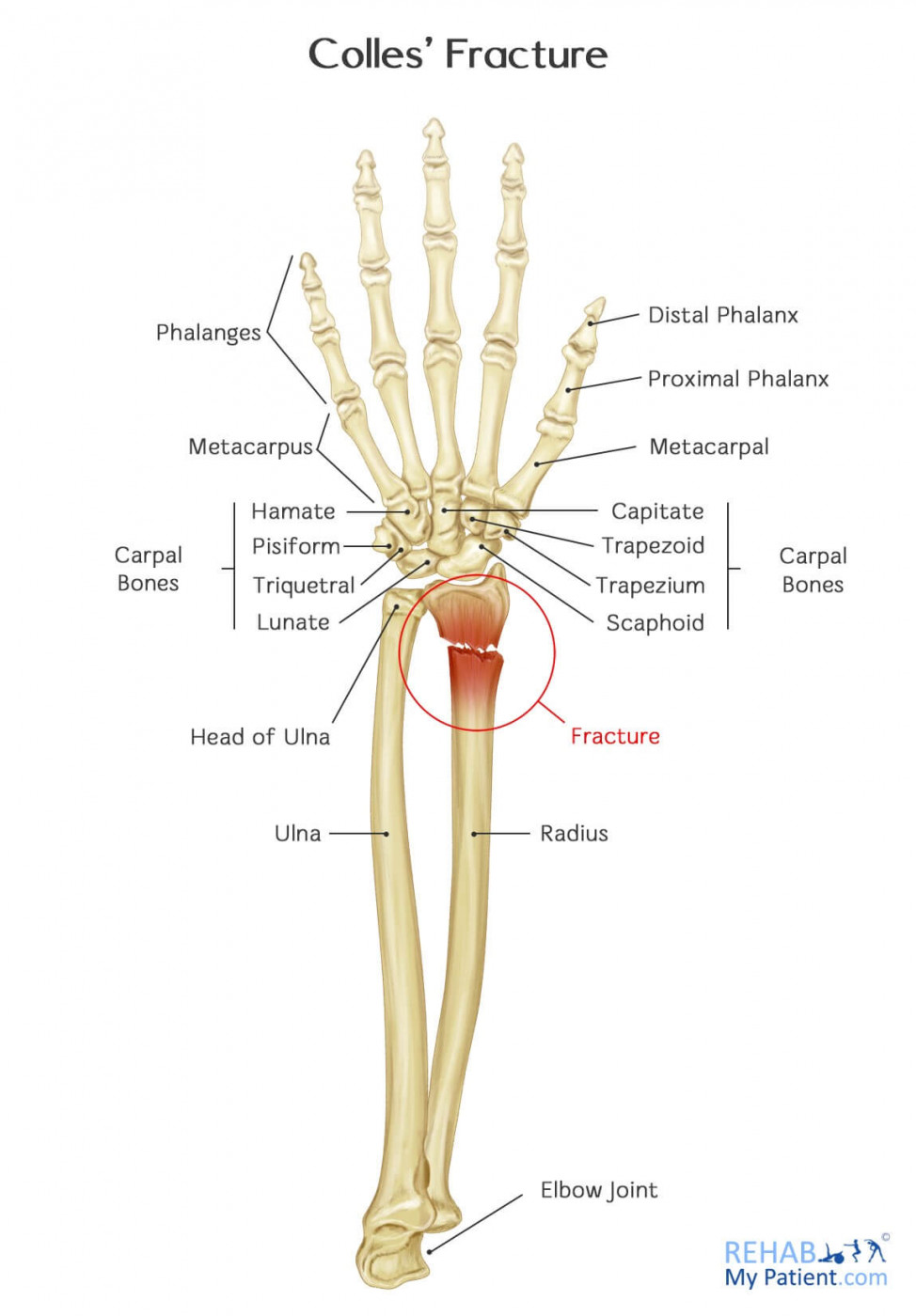
Colles’ fracture of the Radius
Related Subjects: |Shoulder Anterior Dislocations |Shoulder: Posterior Dislocation |Elbow Dislocation |Olecranon Fracture |Distal Humerus Fracture |Radial Head and Neck Fractures |Forearm Fractures |Shaft of Ulna Fracture |Wrist Colles Fracture |Wrist Smith’s Fracture
💥 A Colles’ fracture is a fracture of the distal radius with dorsal displacement, classically following a fall on an outstretched hand (FOOSH). 👉 Common in elderly patients, particularly those with osteoporosis.
🩺 Clinical Features
- Deformity: Classic “dinner-fork” appearance with dorsal wrist swelling.
- Pain & Tenderness: Over distal radius, worsens with wrist movement.
- Neurological Assessment: Check:
- Median nerve: Thenar function, sensation over palmar thumb/index.
- Radial nerve: Wrist extension, sensation over dorsal web space.
- Ulnar nerve: Finger abduction/adduction, sensation over little finger border.
- Vascular Assessment: Check radial & ulnar pulses, capillary refill, and hand perfusion.

🩻 X-Ray Findings
- Fracture: Distal radius with dorsal displacement/angulation.
- Impaction: On AP, radial styloid should be ~1 cm distal to ulnar styloid.
- Angulation: On lateral, normal joint line tips forward by ~5°. If tilted backwards >10°, manipulation is indicated.
🛠️ Management
- Analgesia: Ensure adequate pain relief.
- Immobilisation:
- Apply a wrist splint or below-elbow backslab.
- Broad arm sling for comfort.
- Referral: Stable fractures can be referred to the Virtual Fracture Clinic (VFC).
✋ Indications for Manipulation
- Displacement of the ulnar styloid.
- Impaction: radial styloid < 1 cm distal to ulnar styloid.
- Angulation: dorsal tilt >10° (i.e., >15° from normal volar tilt).
- Distal neurological deficit on exam.
Colles’ fractures are manipulated to preserve wrist function. If patient is unfit for GA, manipulation can be done under procedural sedation in ED. All requiring manipulation must be referred to on-call orthopaedics.
⚠️ Complications
- Malunion → persistent deformity & functional loss.
- Median nerve compression (carpal tunnel syndrome).
- Ulnar styloid fracture non-union.
- Stiffness and complex regional pain syndrome (CRPS).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery