
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Abducent Nerve (Cranial Nerve VI)
Related Subjects:
|Olfactory Nerve
|Optic Nerve
|Oculomotor Nerve
|Trochlear Nerve
|Trigeminal Nerve
|Abducent Nerve
|Facial Nerve
|Vestibulocochlear Nerve
|Glossopharyngeal Nerve
|Vagus Nerve
|Accessory Nerve
|Hypoglossal Nerve
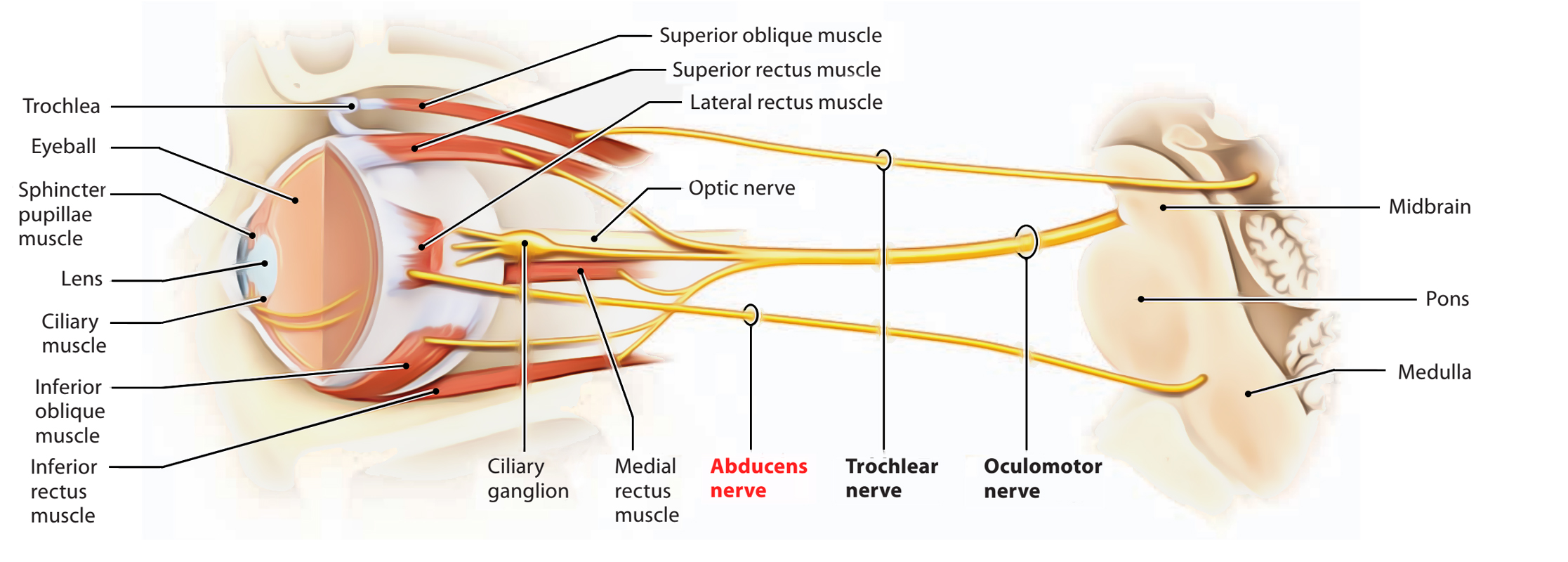
An ipsilateral VIIth nerve palsy alongside a VIth nerve palsy localises the lesion to the pons (facial colliculus).The abducent nerve (cranial nerve VI) is a pure motor nerve. It supplies the lateral rectus muscle, enabling abduction of the eye.
A sixth nerve palsy causes horizontal diplopia worse on gaze toward the affected side, due to failure of lateral rectus function. The affected eye rests medially (unopposed medial rectus). The abducens nerve has a long intracranial course from the pons, over the clivus, through the cavernous sinus, making it particularly vulnerable to raised intracranial pressure and compressive lesions.
In adults, an isolated sixth nerve palsy with vascular risk factors is commonly microvascular, but imaging is warranted if there are red flags (young age, progressive symptoms, bilateral involvement, other cranial nerve deficits). Bilateral sixth nerve palsies should raise immediate concern for raised intracranial pressure. Always examine for papilloedema and assess for associated brainstem or cavernous sinus signs.
🔬Anatomy
Function
🩺 Clinical Features
👁️ Abducens Nerve (VI) Palsy – Causes & Management
Cause 🧩
Typical Features 🔍
Immediate Management 🚑
Definitive / Ongoing Management 🏥
Microvascular ischaemia (diabetes, hypertension) 🩺
Isolated palsy in older patient; vascular risk factors
Exclude red flags; consider MRI if atypical
Optimise vascular risk; usually resolves in 6–12 weeks
Raised intracranial pressure ⚠️
Headache, papilloedema, possibly bilateral palsy
Urgent neuroimaging; assess for papilloedema
Treat underlying cause (mass, hydrocephalus, IIH)
Brainstem infarction 🧠
Associated facial weakness or long-tract signs
Activate stroke pathway
Secondary stroke prevention
Cavernous sinus pathology 🧠
Multiple cranial nerve deficits (III, IV, V1, V2, VI)
Urgent MRI ± MRV
Antibiotics (if thrombosis), anticoagulation, oncology referral
Petrous apex lesion (Gradenigo syndrome) 🦴
Otitis media + facial pain (V1) + VI palsy
ENT referral; imaging temporal bone
IV antibiotics ± surgical drainage
Trauma 🚗
Head injury; skull base fracture
CT head
Neurosurgical management if required
Tumour 🎗️
Progressive symptoms; may involve other cranial nerves
MRI brain
Oncology / neurosurgical management
Inflammatory / demyelinating (e.g. MS) 🔥
Younger patient; other neurological signs
MRI brain with contrast
Steroids if inflammatory; disease-modifying therapy
Myasthenia gravis 💪
Fluctuating diplopia; pupils normal
AChR antibodies; bedside ice test
Pyridostigmine ± immunotherapy
Idiopathic (often post-viral) 🌡️
Isolated palsy in child; recent infection
Imaging to exclude structural cause
Observation if benign cause confirmed
⚡ Practical Approach
🔎 Investigations
💊 Management
References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery