📌 Related Subjects:
Hyperkalaemia
|
ECG - Hyperkalaemia
|
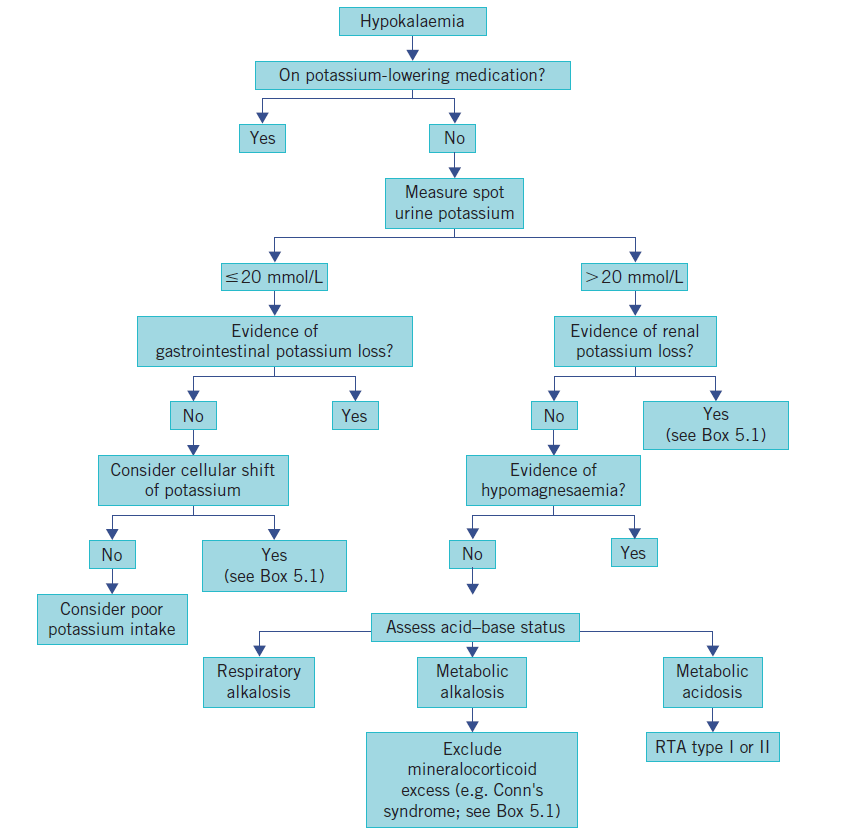
Hypokalaemia
|
Hyperkalaemic and Hypokalaemic Periodic Paralysis
|
Resuscitation - Advanced Life Support
|
Action Potential
📖 Introduction
⚠️ Rapid IV infusions of potassium (K⁺) can be harmful and must be given in a controlled, monitored setting.
Infusion rates should not exceed 40 mmol in 1 L over 4–6 hours unless life-threatening arrhythmia or profound hypokalaemia is present → manage in CCU/HDU.
🩺 Initial Management
- 🏥 Admit to monitored setting, ABC assessment, telemetry.
- 💉 IV N-Saline + 40 mmol/L KCl over 4h via infusion pump if severe.
- 💊 Oral supplementation: Sando-K 2–3 tablets BD/TDS if tolerated.
- ⚡ Correct coexistent hypomagnesaemia.
- 🚫 Avoid loop diuretics if possible.
- ❤️ Increased arrhythmia risk with low Mg²⁺, long QT, or digoxin use.
🔎 Causes (with clinical notes & management)
- ⚡ Diuretics (Loop/Thiazide)
Symptoms: weakness, cramps, arrhythmias (U waves, flat T).
Ix: U&E, Mg²⁺, ECG.
Tx: K⁺ replacement, correct Mg²⁺, adjust/stop diuretic.
- 🤢 GI Losses (Vomiting, Diarrhoea)
Symptoms: dehydration, hypotension, arrhythmias.
Ix: U&E, bicarbonate, stool studies.
Tx: Rehydration, oral/IV K⁺, antiemetic/antidiarrhoeal.
- 🧬 Hyperaldosteronism
Symptoms: hypertension, cramps, metabolic alkalosis.
Ix: U&E, renin/aldosterone, adrenal imaging.
Tx: Spironolactone; surgery if adrenal adenoma.
- ⚡ Magnesium Deficiency
Features: cramps, arrhythmias, ↑ neuromuscular irritability.
Ix: Mg²⁺, K⁺, ECG.
Tx: Replace Mg²⁺ (essential for K⁺ correction).
- 💉 Insulin Administration
Features: cramps, arrhythmias due to K⁺ shift into cells.
Ix: K⁺, glucose, ECG monitoring.
Tx: Supplement K⁺, adjust insulin dose if possible.
🤒 Clinical Features
- Weakness, palpitations, lethargy.
- Severe: arrhythmias (torsades de pointes), heart failure, rhabdomyolysis.
- May cause diaphragmatic weakness → respiratory compromise.
🔬 Investigations
- U&E: normal range 3.5–5.0 mmol/L; moderate 2.5–3.0; severe <2.5.
- Check Ca²⁺, Mg²⁺, venous HCO₃⁻.
- ECG: U waves, ST depression, prolonged QT.
- Other tests guided by underlying cause.
💊 Management
- ✅ ABC, IV fluids as needed, treat cause.
- 😷 Mild–moderate: oral K⁺ replacement (Sando-K).
- ⚡ Severe (<2.5 or arrhythmia): IV K⁺ via central line in CCU/HDU.
- 🧮 Sympathetic states (e.g., theophylline toxicity): propranolol may help.
📚 References
