
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Urinary Tract Obstruction
Related Subjects: |Renal Transplantation |Urinary Tract Obstruction
🚨 Obstructive Uropathy = any blockage of urine flow between the renal collecting ducts and the urethral meatus. 👉 Unilateral ureteric obstruction usually causes no detectable change in urine flow or creatinine. 👉 Renal failure develops only when both kidneys are obstructed or in patients with a single functioning kidney.
ℹ️ About
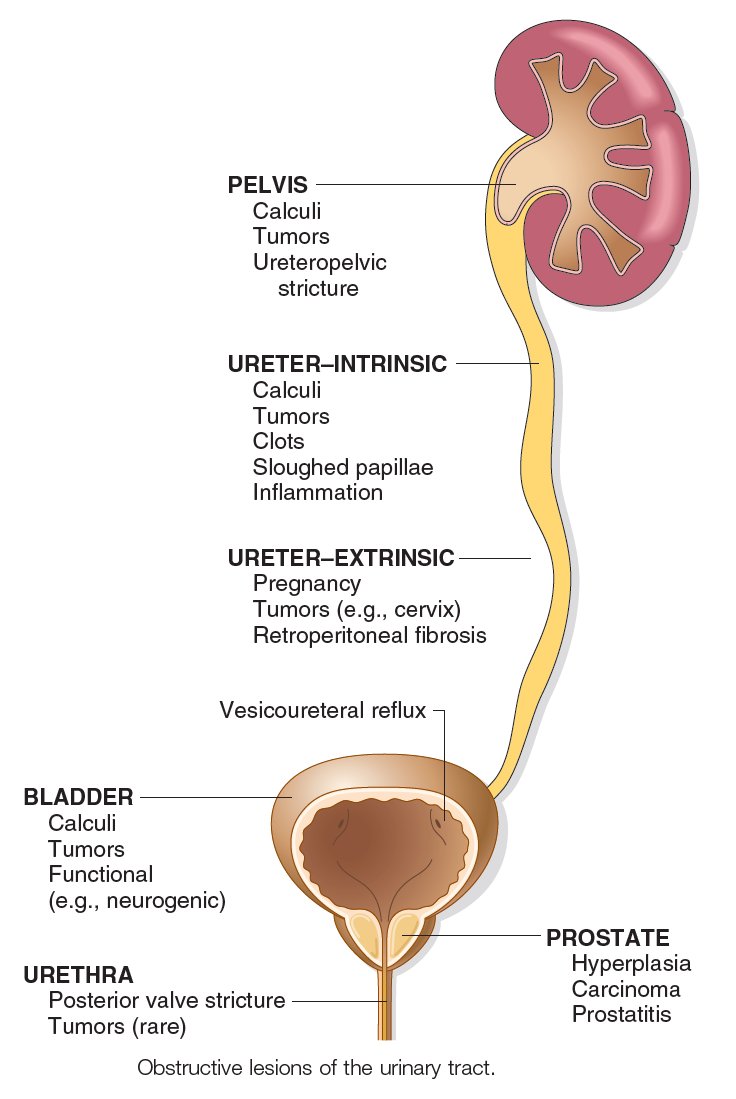
- Obstruction can occur anywhere from collecting ducts → urethral meatus.
- 🖼️ Imaging usually shows dilatation proximal to obstruction (hydronephrosis, hydroureter).
- ⚠️ Chronic obstruction may cause irreversible renal damage.
🧬 Causes
- Renal: Papillary necrosis, staghorn calculus, tumour, clot.
- Ureteric: Stone, extrinsic tumour (e.g. cervical, colorectal), intrinsic tumour, retroperitoneal fibrosis.
- Bladder: Calculi, tumour, clot, neuropathic bladder, retention (e.g. constipation).
- Urethral: Prostatic hypertrophy, prostate cancer, urethral stricture, stone, phimosis.
🩺 Clinical Presentation
- 🔺 AKI: ↑ creatinine, metabolic acidosis, hyperkalaemia.
- Above bladder: Flank pain, fullness.
- Partial bladder outlet obstruction: Hesitancy, weak stream, polyuria, nocturia.
- At/below bladder: Acute retention, painful distended bladder.
- Exam: Palpable bladder, DRE may show enlarged prostate or hard stool.
🔎 Investigations
- 🧪 Bloods: FBC, U&E → AKI, metabolic acidosis, hyperkalaemia.
- 🖥️ Ultrasound: First-line, shows hydronephrosis/hydroureter, identifies obstruction level.
- CT urogram / spiral CT if unclear cause.
- Radionuclide scan (MAG3/DTPA) if function assessment required.
- Bladder scan → postvoid residual >200 mL = abnormal, suggests outlet obstruction.
💡 Post-Obstructive Diuresis: After relief of obstruction, patients may pass very high volumes of urine due to retained sodium/urea and impaired concentrating ability. 👉 Requires close monitoring and IV fluid replacement to prevent hypovolaemia and electrolyte disturbance.
🛠️ Management
- 🚑 Immediate: Catheterisation in retention, monitor urine output.
- 📡 Identify level: Ultrasound ± further imaging to determine site & cause.
- ⚠️ Monitor: Watch for post-obstructive diuresis, correct with fluids and electrolytes.
- 👨⚕️ Male BOO: α1-blocker (tamsulosin) or 5α-reductase inhibitor (finasteride). TURP if severe/progressive.
- 🩺 Definitive: Stent insertion, nephrostomy, or surgery depending on cause (e.g. stone removal, tumour resection, fibrosis release).
💡 Exam Pearls:
• Always check for reversible causes (stones, prostate).
• Unilateral obstruction = no creatinine rise; bilateral obstruction = AKI.
• Post-obstructive diuresis is a common viva question – fluids must match output.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery