
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Spleen
|Anatomy of the Ear |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the SpleenThe spleen is the largest secondary lymphoid organ and a highly vascular “blood filter” in the left upper quadrant. It removes senescent or abnormal red cells and platelets, mounts immune responses to blood-borne pathogens, and acts as a reservoir for immune cells (notably monocytes). Its unique microanatomy (red pulp + white pulp) explains classic clinical findings such as Howell–Jolly bodies after splenectomy and the susceptibility to encapsulated organisms.
Anatomy of the Spleen
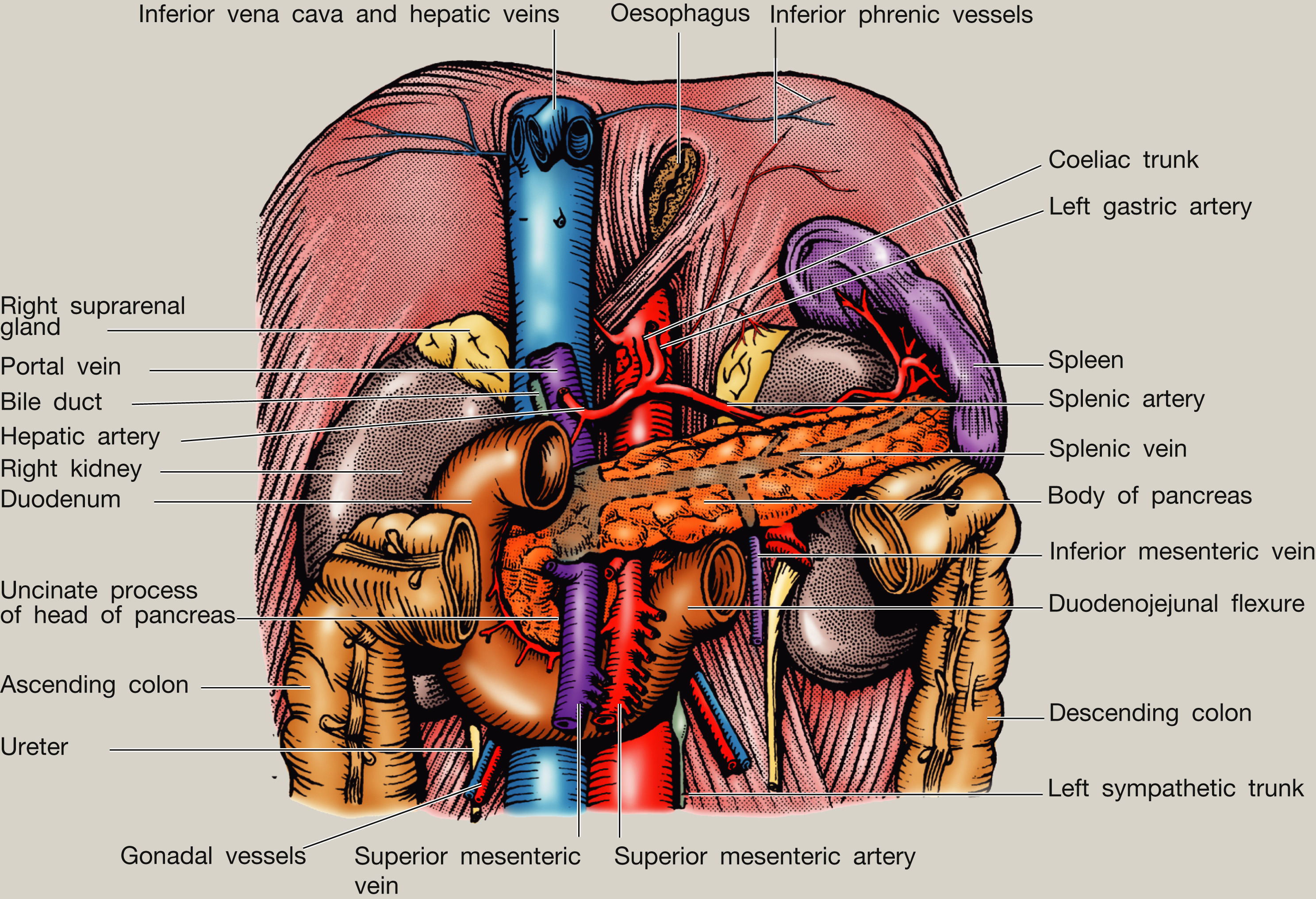
Relations
1) Gross Anatomy
- Location: left hypochondrium, deep to ribs 9–11, under the left hemidiaphragm; long axis parallels the 10th rib.
- Shape: ovoid, soft, highly vascular organ with a notched anterior border (helpful on palpation when enlarged).
- Peritoneal status: intraperitoneal (except at the hilum), suspended by peritoneal ligaments.
- Key relations:
- Anterior: stomach (via gastrosplenic ligament).
- Medial: tail of pancreas approaches the hilum.
- Inferior: left colic flexure.
- Posterior: left kidney and diaphragm (splenic pain may be referred to shoulder via diaphragm irritation).
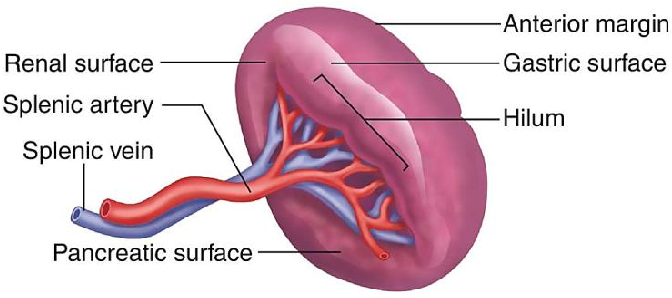
2) Ligaments and the Hilum
- Gastrosplenic ligament: between stomach and spleen; contains short gastric and left gastro-omental vessels.
- Splenorenal (lienorenal) ligament: between spleen and left kidney; contains the splenic artery/vein and tail of pancreas.
- Hilum: entry/exit for splenic vessels, lymphatics, and nerves.
3) Blood Supply and Venous Drainage 🩸
The spleen has a high blood flow and a “slow circulation” through cords and sinusoids, ideal for quality-control of red cells but making it vulnerable to haemorrhage if injured.
- Arterial supply: splenic artery (branch of the coeliac trunk), characteristically tortuous along the superior border of the pancreas.
- Venous drainage: splenic vein → joins SMV to form the portal vein.
4) Lymphatic Drainage and Innervation
- Lymphatics: drain to pancreaticosplenic nodes → coeliac nodes.
- Innervation: sympathetic fibres via the coeliac plexus (vasomotor control); pain often relates to capsular stretch.
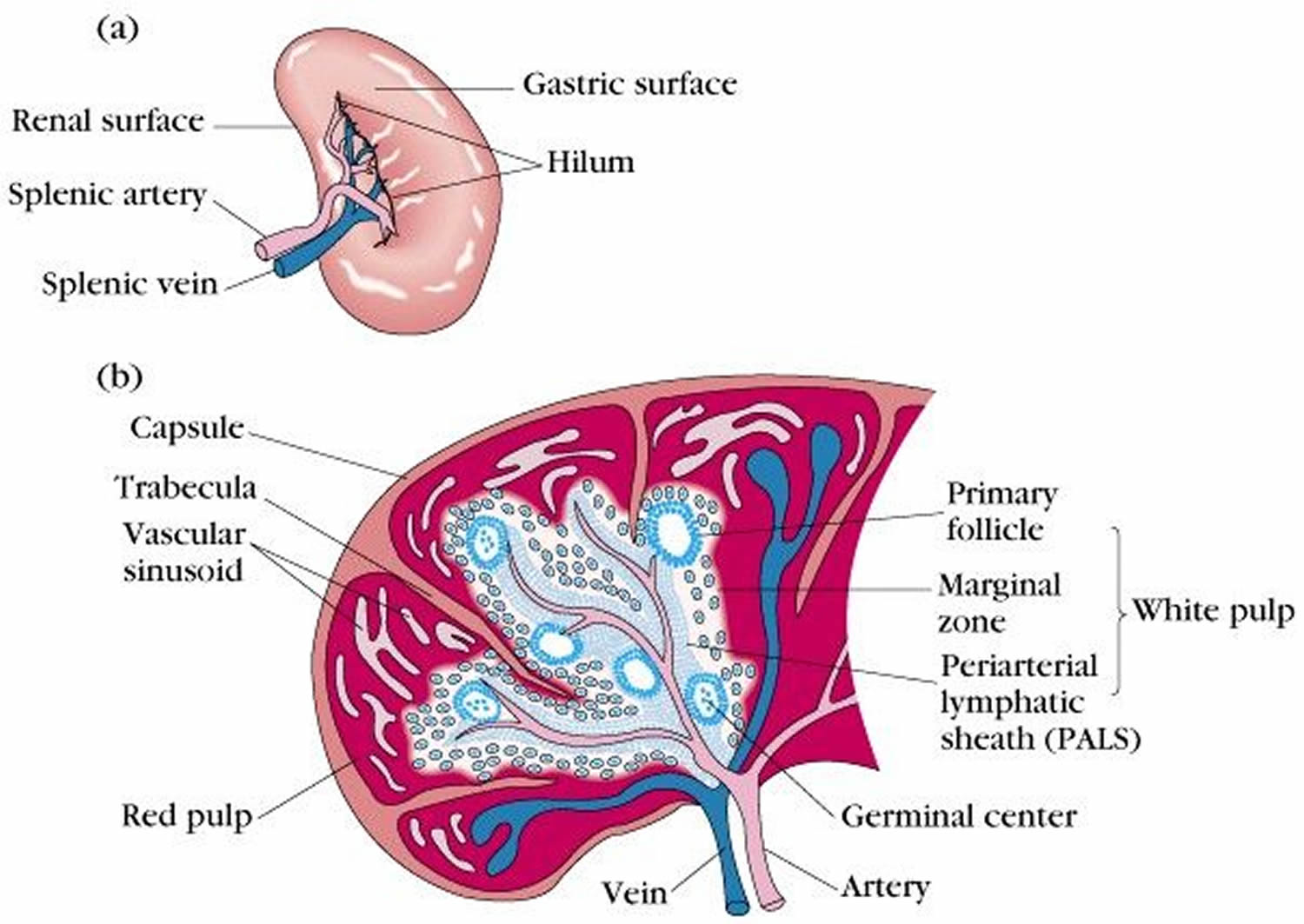
5) Microanatomy (Why Red Pulp and White Pulp Matter)
- Capsule + trabeculae: fibrous capsule sends trabeculae inward, carrying vessels and providing structure.
- White pulp (immune):
- Organised around central arterioles.
- PALS (periarteriolar lymphoid sheath) is T-cell rich.
- Lymphoid follicles are B-cell rich; can form germinal centres during immune activation.
- Marginal zone: interface that “samples” blood antigens; rich in macrophages and specialised B cells (critical for encapsulated bacteria responses).
- Red pulp (filtration):
- Splenic cords (of Billroth): meshwork of macrophages and cells where blood slows.
- Sinusoids: endothelial-lined channels; RBCs must deform to pass through-rigid/abnormal cells are trapped and removed.
Physiology of the Spleen
1) Blood Filtration and “Quality Control” of Red Cells
- Culling: removal of senescent, rigid, or damaged RBCs (e.g., spherocytes) by macrophages.
- Pitting: removal of RBC inclusions (e.g., nuclear remnants); absence of spleen → Howell–Jolly bodies appear on blood film.
- Iron recycling: haemoglobin breakdown → iron salvaged and returned to marrow/liver for reuse; bilirubin generated from haem metabolism.
2) Immune Surveillance of Blood-borne Pathogens 🛡️
- Phagocytosis: macrophages clear opsonised bacteria and immune complexes from circulation.
- Antibody responses: B cells in white pulp generate antibodies (important for polysaccharide capsules).
- Memory formation: contributes to longer-term immune protection against recurrent exposures.
3) Platelet and Cell Sequestration
- The spleen normally sequesters a proportion of platelets and can increase pooling when enlarged.
- Clinical: splenomegaly can contribute to thrombocytopenia via increased sequestration and destruction.
4) Reservoir Function (Species- and Context-dependent)
- The spleen can act as a reservoir for immune cells (notably monocytes), mobilised during inflammation or tissue injury.
- It can hold blood volume, but in humans this “emergency transfusion” role is less dramatic than in some animals.
5) Haematopoiesis (When Marrow Can’t Cope)
- Fetal life: contributes to haematopoiesis before marrow fully takes over.
- Extramedullary haematopoiesis: in adults with marrow failure or high demand (e.g., myelofibrosis, severe haemolytic anaemia) → splenic enlargement.
Clinical Relevance
1) Splenomegaly
- Mechanisms: congestion (portal hypertension), increased workload (haemolysis), infiltration (malignancy/storage disease), infection/inflammation.
- Symptoms/signs: LUQ fullness, early satiety (gastric compression), pain from capsular stretch; may see cytopenias if hypersplenism develops.
2) Hypersplenism
- Definition (functional concept): splenic overactivity → excessive sequestration/destruction → cytopenias (anaemia, leukopenia, thrombocytopenia) often with an enlarged spleen.
- Management principle: treat underlying cause; splenectomy is reserved for selected cases due to infection risk.
3) Asplenia / Hyposplenia (Why It Matters)
- Risk: increased susceptibility to severe infection, especially from encapsulated bacteria (classically pneumococcus, Hib, meningococcus).
- Blood film clues: Howell–Jolly bodies; target cells may be seen.
- Prevention: vaccinations + patient education; some patients need prophylactic antibiotics depending on local policy and risk profile.
4) Splenic Rupture (Trauma and Beyond)
- Why dangerous: highly vascular organ → life-threatening intra-abdominal bleeding.
- Presentation: LUQ pain, peritonism, shock; referred left shoulder tip pain can occur (diaphragmatic irritation).
- Management: depends on haemodynamic stability (non-operative management vs embolisation vs surgery).
✅ Summary
The spleen is a highly vascular lymphoid organ that combines immune surveillance (white pulp) with blood filtration and red cell “quality control” (red pulp). Its architecture forces RBCs to deform through sinusoids-trapping rigid or abnormal cells for macrophage clearance and iron recycling. Clinically, splenic enlargement reflects congestion, haemolysis, infiltration, or infection, while loss of splenic function increases vulnerability to severe infections with encapsulated organisms.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery