Related Subjects:
|Anti-NMDA (NMDAR) receptor encephalitis
|Herpes Simplex Encephalitis (HSV)
|Acute Encephalitis
|Limbic Encephalitis
|Paraneoplastic Limbic Encephalitis (Dementia)
|Hashimoto's (Steroid responsive) Encephalopathy
|Acute Disseminated Encephalomyelitis
|Measles
|Lumbar Puncture
|CSF Interpretation
|Acute Hydrocephalus
🚨 Acute Hydrocephalus is a neurological and neurosurgical emergency requiring rapid recognition and urgent intervention. Delay can result in brain herniation and death.
🔎 Aetiology & CSF Physiology
- Normal CSF volume ≈ 200 mL, produced mainly by the choroid plexus (~500 mL/day; ~20 mL/hr).
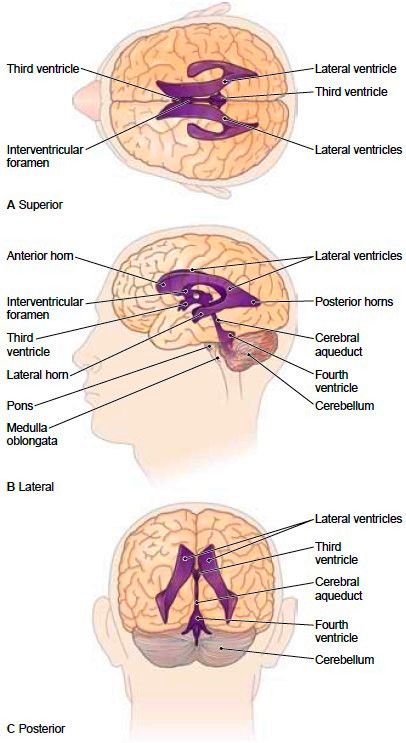
- CSF flows: Lateral ventricles → Third ventricle → Fourth ventricle → Subarachnoid space via foramina of Luschka & Magendie.
- Absorption via arachnoid granulations into dural venous sinuses.
- Hydrocephalus: Excess CSF accumulation → ventricular dilation → increased intracranial pressure (ICP) and brain compression.
- Incidence: ~1–2 per 1,000 live births (congenital), adults uncommon but often secondary to tumour, haemorrhage, infection, or post-surgery.
- Types:
- Communicating hydrocephalus: Blockage of absorption (e.g., post-SAH, meningitis, carcinomatous meningitis).
- Obstructive / Non-communicating hydrocephalus: Blockage within ventricular system (e.g., aqueduct stenosis, colloid cyst, tumour, Chiari malformation, Dandy-Walker).
- Normal Pressure Hydrocephalus (NPH): Chronic adult form; triad: gait disturbance, dementia, urinary incontinence.
🧠 Ventricular Anatomy
👶 Clinical Features in Infants
- Rapid head enlargement due to open fontanelles; head circumference >2 SD above mean.
- “Sun-setting eyes” 👀 – upward gaze limitation from tectal pressure.
- Irritability, vomiting, poor head control, tense/tense fontanelle, thin shiny scalp.
- Delayed developmental milestones, hypotonia, breathing irregularities.
- Seizures may occur in severe or obstructive cases.
👩🦳 Clinical Features in Older Children & Adults
- Severe headache, nausea, vomiting, blurred vision, papilloedema.
- Gait disturbance, truncal ataxia, UMN signs (spasticity, hyperreflexia).
- Pituitary dysfunction if suprasellar pressure (amenorrhea, hypothyroidism).
- False-localising VI nerve palsy, impaired upward gaze (3rd ventricle enlargement).
- Severe cases: reduced consciousness, coma, pupillary changes, Cheyne-Stokes respiration.
🧪 Investigations
- CT Head: First-line in acute hydrocephalus; shows ventricular dilation, mass effect, and obstructive lesions.
- MRI Brain: More sensitive for aqueduct stenosis, posterior fossa lesions, or congenital malformations.
- Patterns: Symmetrical enlargement in communicating hydrocephalus; obstructive hydrocephalus shows upstream dilation with normal downstream ventricles.
- ICP monitoring may be used in ICU if severe or unstable.
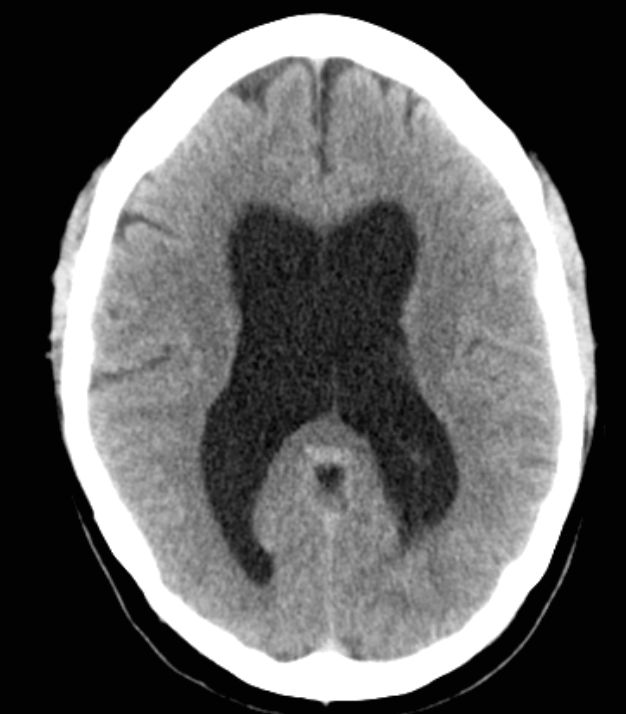
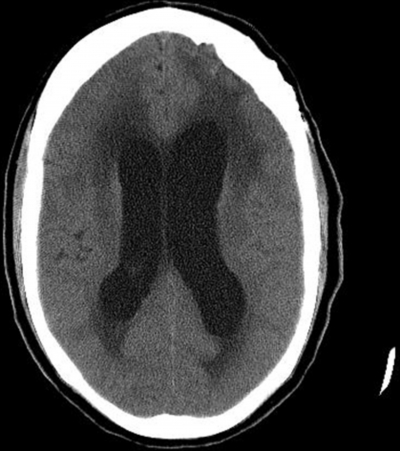
📸 Classical Imaging Signs
- Dilated lateral and third ventricles; temporal horn enlargement.
- Convex third ventricular walls; rounded frontal horns.
- Effaced cortical sulci; disproportionate ventricular enlargement relative to cortical atrophy.
- Periventricular white matter hypodensity (transependymal CSF flow) in chronic cases.
⚡ Management
- Emergency neurosurgical referral is mandatory.
- Surgical Options:
- External Ventricular Drain (EVD): Temporary CSF diversion; allows ICP monitoring; used in acute obstructive hydrocephalus, post-hemorrhage or infection.
- Ventriculoperitoneal (VP) Shunt: Permanent CSF diversion to peritoneum; first-line in chronic or communicating hydrocephalus.
- Endoscopic Third Ventriculostomy (ETV): Internal diversion; preferred in obstructive hydrocephalus (e.g., aqueduct stenosis) when anatomy suitable.
- Medical management (bridging therapy): Acetazolamide or furosemide to reduce CSF production; used only while awaiting surgery.
- Supportive care: Elevate head of bed, monitor vitals, osmotic therapy if raised ICP (mannitol/ hypertonic saline under ICU supervision).
- Complications: Shunt infection or obstruction, subdural hematoma, shunt fracture/disconnection, overdrainage.
🖼️ Imaging Examples

📝 Student / Exam Tips
- ⚡ Acute headache + nausea/vomiting + papilloedema → suspect acute hydrocephalus.
- 👶 In infants, measure head circumference and assess fontanelles; “sun-setting eyes” = red flag.
- 🧠 Identify obstructive vs communicating hydrocephalus on imaging (upstream dilation, effaced sulci).
- 🚑 Immediate neurosurgical input is required; do not delay for MRI if patient unstable.
- 💊 Medical therapy is temporary; definitive treatment is surgical.
- 📚 NPH triad (gait disturbance, dementia, incontinence) is exam favourite in adult chronic hydrocephalus.
📚 References / Guidelines
