
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Neonatal meningitis
Related Subjects: |Lumbar Puncture |CSF Interpretation |CSF Rhinorrhoea
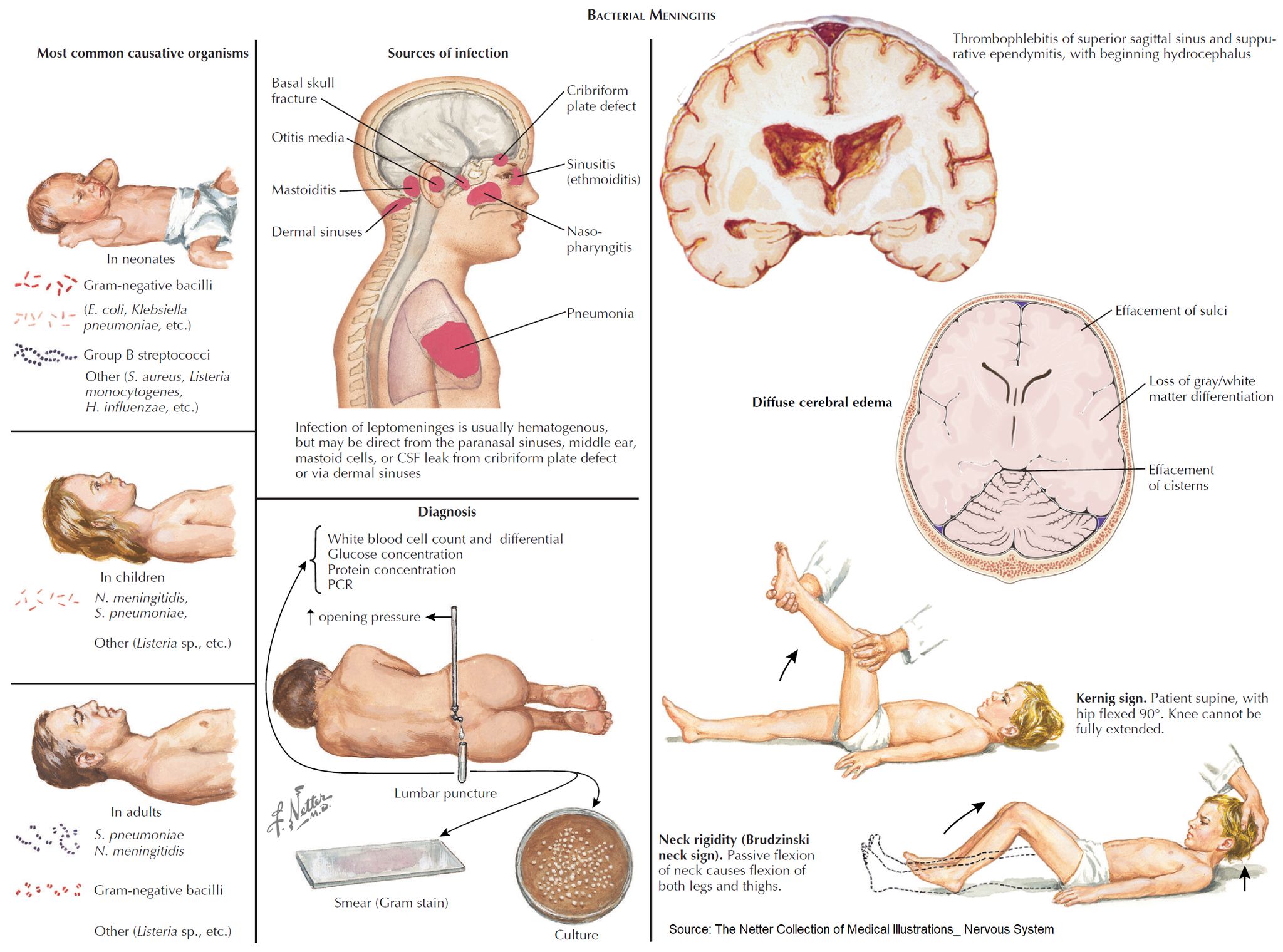
👶🧠 Neonatal meningitis – Definitive diagnosis is made by CSF examination via lumbar puncture (LP). LP should be performed in any neonate suspected of sepsis/meningitis, but ⚠️ treatment must not be delayed while awaiting results.
📖 About
- Occurs within the first 90 days of life 🍼.
- Most often bacterial, and is a life-threatening emergency 🚨.
🩺 Clinical Presentation
- ⚠️ Classical triad (fever, stiff neck, vomiting) often absent.
- Instead look for:
- ❌ Poor feeding, irritability, lethargy
- 😴 Apnoea, listlessness, reduced tone
- 🌡️ Fever OR hypothermia
- ⚡ Seizures
- 🚩 Other red flags: bulging fontanelle, high-pitched cry, hypoglycaemia, metabolic acidosis, shock, pallor
🦠 Microbiology
- Group B Streptococcus (GBS) 🧬 → ~50% (esp. type III; vertical transmission).
- Escherichia coli (K1 capsule) 🦠 → ~20%.
- Listeria monocytogenes 🥗 → 5–10% (contaminated food in pregnancy).
- Viruses 🦠 → HSV, VZV (less common, but important for prognosis).
⚠️ Complications
- ♿ Cerebral palsy (~8%)
- 📘 Learning disability (~7%)
- ⚡ Persistent seizures (~7%)
- 👂 Hearing loss (~25%)
- 🧠 Hydrocephalus, abscess, or subdural effusion
👶➡️👧 Causes in Older Infants (>3 months)
- Streptococcus pneumoniae 🧬
- Neisseria meningitidis 💉
- Haemophilus influenzae type b (Hib) 💊 (much less common since vaccination).
💊 Management
- 🚑 Immediate IV antibiotics (before LP if unstable):
- Ampicillin + Cefotaxime (UK NICE guidance) 💉
- Avoid ceftriaxone in neonates (risk of kernicterus) ❌
- 💧 Supportive care: fluids, oxygen, seizure control (phenobarbital/levetiracetam).
- 🦠 If HSV suspected: add Acyclovir 🧪
- 🔊 Hearing test follow-up (due to high risk of deafness).
- 🧪 Close monitoring: blood cultures, CSF studies, CRP trends.
- 👩👦 Public health: maternal screening & prophylaxis for GBS at delivery reduces risk.
🧑🏫 Exam Tip
Neonatal meningitis is one of the few conditions where the common organisms differ significantly from older children. Always think GBS, E. coli, and Listeria 👶 - whereas after 3 months, pneumococcus and meningococcus dominate.
Cases - Neonatal Meningitis
- Case 1 - Early-onset GBS infection 🍼: A 3-day-old term infant presents with poor feeding, irritability, and fever. Exam: bulging fontanelle, lethargy. CSF: neutrophilia, low glucose, high protein. Blood culture: Group B Streptococcus. Diagnosis: early-onset neonatal meningitis (GBS). Managed with IV benzylpenicillin + gentamicin, then tailored antibiotics.
- Case 2 - E. coli meningitis 🦠: A 10-day-old preterm baby develops temperature instability, seizures, and poor tone. Mother had prolonged rupture of membranes. CSF: Gram-negative bacilli, low glucose, high protein. Culture: E. coli K1. Diagnosis: neonatal meningitis due to E. coli. Managed with IV cefotaxime for 21 days.
- Case 3 - Listeria infection 🥛: A 14-day-old infant presents with poor feeding, apnoea, and irritability. Mother ate unpasteurised cheese during pregnancy. CSF: mononuclear predominance, positive Gram-positive bacilli. Diagnosis: Listeria monocytogenes meningitis. Managed with IV ampicillin + gentamicin.
Teaching Point 🩺: Neonatal meningitis is most often caused by Group B Strep, E. coli, or Listeria. - Early onset (<7 days): GBS, E. coli, Listeria (maternal transmission). - Late onset (>7 days): same organisms + nosocomial Gram-negatives. Presents non-specifically (poor feeding, irritability, temperature instability, seizures). Management: urgent IV antibiotics + supportive care. Mortality and neurological sequelae remain high.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery