
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Central Spinal Cord Syndrome
Related Subjects: | Transverse myelitis | Acute Disseminated Encephalomyelitis |Cervical spondylosis |Spinal Cord Anatomy |Acute Disc Prolapse |Spinal Cord Compression |Spinal Cord Haematoma |Foix-Alajouanine syndrome |Cauda Equina |Conus Medullaris syndrome |Anterior Spinal Cord syndrome |Central Spinal Cord syndrome |Brown-Sequard Spinal Cord syndrome
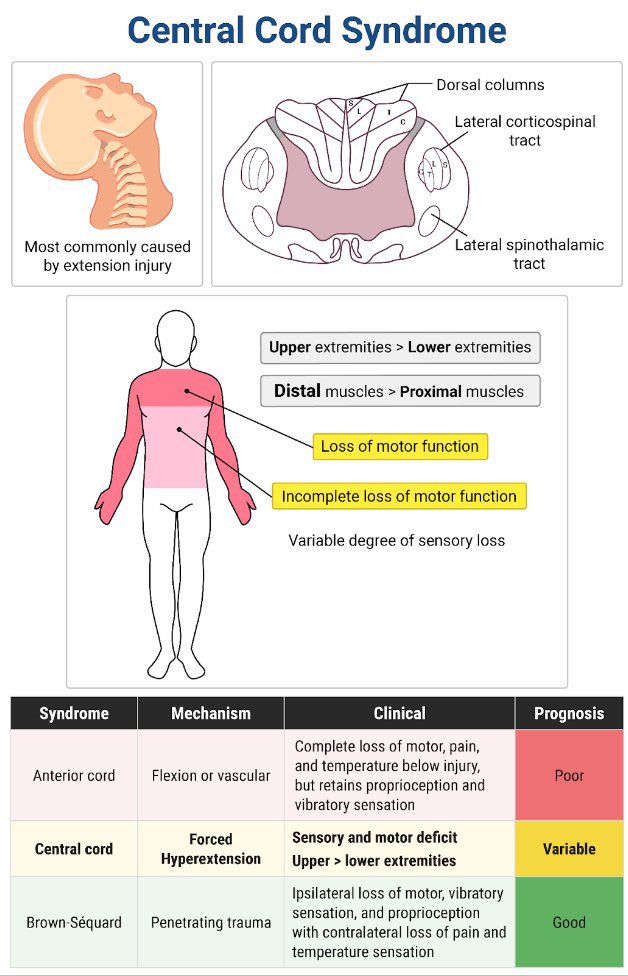
⚠️ Central Cord Syndrome (CCS) is the most common incomplete spinal cord injury.
💡 Classic clue: an older patient after a fall with a forehead or facial bruise, neck pain, and arm weakness that is worse than leg weakness.
🧠 Typically follows a hyperextension injury in the context of pre‑existing cervical spondylosis.
ℹ️ About Central Cord Syndrome
- Results from damage to the central portion of the cervical spinal cord.
- Most commonly caused by neck hyperextension injuries.
- Occurs after falls, road traffic collisions, or sports trauma.
- Strongly associated with cervical canal narrowing from spondylosis.
🔑 Key Red Flags
- 👴 Older patient with facial or forehead bruising following a fall.
- 💪 Disproportionate weakness of upper limbs compared with lower limbs.
- 🧩 “Cape‑like” loss of pain and temperature across shoulders and arms.
- 🚽 Early urinary retention progressing to incontinence.
- ❌ Plain X‑rays or CT may be normal - MRI is essential.
🧠 Relevant Anatomy
- Central cervical cord involvement, particularly corticospinal and spinothalamic tracts.
- Corticospinal tract somatotopy: medial fibres supply upper limbs, lateral fibres supply lower limbs.
- This organisation explains why arm weakness is more severe than leg weakness.
- Spinothalamic tract involvement causes a cape‑like sensory deficit.
🧬 Aetiology & Pathophysiology
- Hyperextension causes cord compression between anterior osteophytes and posterior ligamentum flavum.
- Anterior spinal artery hypoperfusion may contribute to central cord ischaemia.
- Fracture or dislocation may be absent.
- Autonomic dysreflexia can occur if injury is above T6.
🩺 Clinical Features
- 💪 Arm weakness greater than leg weakness - patients may walk but struggle with fine motor tasks (“walking but not writing”).
- 🧩 Loss of pain and temperature sensation in a cape distribution.
- ⚡ Upper motor neurone signs: spasticity, hyperreflexia, clonus.
- 🚽 Bladder dysfunction: acute retention or later incontinence.
- 🔥 Neuropathic pain, especially in upper limbs.
- 😵 Possible Horner’s syndrome with high cervical involvement.
- 🩸 Autonomic dysreflexia: episodic flushing, headache, sweating, and hypertension.
🔎 Investigations
- MRI – gold standard: demonstrates cord oedema, haemorrhage, and ongoing compression.
- CT spine: best for identifying bony injury but may miss cord pathology.
- Electrophysiology: NCS or SSEPs if diagnostic uncertainty remains.
💊 Management
- 🚑 Initial trauma care: ABCs, cervical immobilisation, oxygen, IV access.
- 🧠 Urgent MRI to confirm diagnosis and exclude instability.
- 💊 High‑dose steroids: not routinely recommended (controversial; not advised by NICE).
- 🔪 Surgery if persistent cord compression, instability, or worsening neurology.
- ♿ Rehabilitation: physiotherapy, occupational therapy, bladder and bowel care.
- 💊 Neuropathic pain: gabapentin, pregabalin, TCAs, or SNRIs.
- 💊 Spasticity: baclofen ± botulinum toxin in refractory cases.
- 📚 Education for patients and carers regarding autonomic dysreflexia.
📚 Teaching Pearls
👉 Most common incomplete spinal cord syndrome. 👉 Think CCS in elderly patients with falls and arm weakness out of proportion to leg weakness. 👉 MRI is essential even when CT or X‑ray is normal. 👉 Prognosis: ambulation often recovers, but hand function may remain impaired. 👉 Classic phrase: “Walking but not writing.”
🩺 Clinical Cases
-
Case 1 – Elderly fall with hyperextension:
A 72‑year‑old man falls forward, striking his chin. CT shows cervical spondylosis without fracture. Examination reveals marked upper‑limb weakness, milder leg weakness, brisk reflexes, and preserved sacral sensation.
Teaching point: Central cord syndrome due to hyperextension on a background of cervical canal stenosis is classic in older patients. 🚑 -
Case 2 – High‑energy trauma in a young patient:
A 25‑year‑old motorcyclist sustains neck hyperextension in an RTC. He has significant hand weakness and upper‑limb dysaesthesia, with relatively preserved leg strength. MRI shows cord oedema at C4–C6 without fracture.
Teaching point: CCS can also occur in younger patients after severe trauma. Walking often recovers, but fine hand function may be persistently affected. 🏍️
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery