
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Spontaneous Pneumothorax
Related Subjects: Asthma
|Acute Severe Asthma
|Exacerbation of COPD
|Pulmonary Embolism
|Cardiogenic Pulmonary Oedema
|Pneumothorax
|Tension Pneumothorax
|Respiratory (Chest) infections Pneumonia
|Fat embolism
|Hyperventilation Syndrome
|ARDS
|Respiratory Failure
|Pleural effusion
|Pleural tap (thoracentesis)
⚠️ Treatment depends critically on whether it is a primary or secondary pneumothorax. Underlying lung disease = secondary, which is treated far more cautiously. 💨 Always suspect a pneumothorax in any mechanically ventilated patient with sudden deterioration (may present only as ↑ resistance to ventilation).
📖 About
- 🫁 Spontaneous presence of air in the pleural space.
- 👵 Patients >50 or with lung disease = secondary pneumothorax → require admission.
⚙️ Mechanism
- Hole in visceral pleura → air leaks into pleural space.
- Penetrating wounds (oesophagus, mediastinum, diaphragm).
- Gas-forming bacteria within empyema.
📂 Types
- 🟢 Primary: Age <50, no lung disease, minimal smoking history.
- 🔴 Secondary: Due to underlying lung disease.
- ⚔️ Traumatic: Injury-related (penetrating/blunt).
📊 Classification
- Primary Pneumothorax:
- 👨 Tall, thin young men (20–40 yrs), often right-sided.
- 🚬 Smoking ↑ risk (even subclinical lung disease).
- 🌬️ Subpleural blebs rupture due to apex stress.
- 🔁 Recurrence: ~40% within 2 years (especially smokers).
- Secondary Pneumothorax:
- Due to 👇
- ⚔️ Trauma (penetrating injuries).
- 💉 Iatrogenic (biopsy, pleural procedures).
- 💨 Ventilation (barotrauma with high PEEP).
- 🫁 Lung disease (COPD, asthma, CF, PCP pneumonia).
- 📉 Rare: Marfan’s, catamenial (endometriosis).
- Due to 👇
🩺 Clinical
- May be silent if small.
- Typical: sudden chest pain ⚡ + breathlessness 🫁.
- Severe: hypotension, tachycardia, cyanosis.
- Exam: hyper-resonance, ↓ breath sounds. ➡️ Tension PTX: tracheal deviation + distended neck veins.
🔍 Investigations
- 📸 CXR: Lung edge visible, no markings peripheral to it.
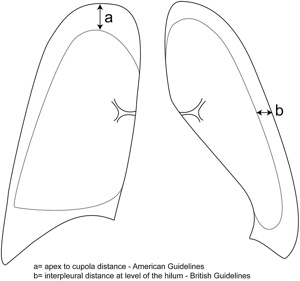
- 📏 Size: Small = <2 cm rim; Large = >2 cm.
- 🖥️ HRCT: For complex cases / to differentiate bullae.
💊 Management of Spontaneous Pneumothorax
- Initial assessment: ABCDE assessment, observations, oxygen saturation, analgesia and chest X-ray. Give oxygen if hypoxic; use controlled oxygen in patients at risk of CO₂ retention, such as severe COPD. If tension pneumothorax is suspected clinically, treat immediately — do not wait for imaging. Assess: symptoms, haemodynamic stability, oxygen requirement, underlying lung disease, pneumothorax size and recurrence risk.
- Size terminology: Older BTS guidance used a 2 cm rim on CXR at the level of the hilum to define a large pneumothorax. Current practice is more symptom-led: breathlessness, physiological compromise and underlying lung disease often matter more than size alone. A small pneumothorax is often described as <2 cm; a large pneumothorax as ≥2 cm, but management should not rely on size alone.
- Primary Spontaneous Pneumothorax
- No underlying lung disease: Minimally symptomatic and physiologically stable: consider conservative management, even if large, with safety-netting and early follow-up.
- Symptomatic or patient prefers active treatment: consider needle aspiration, ambulatory device or small-bore chest drain depending on local expertise and patient preference.
- Failed aspiration, persistent symptoms, ongoing air leak or clinical deterioration: insert a small-bore chest drain and admit.
- Secondary Spontaneous Pneumothorax — underlying lung disease, e.g. COPD, asthma, cystic fibrosis, ILD:
- Lower threshold for admission because respiratory reserve is reduced.
- Small and minimally symptomatic: admit for observation, oxygen if needed, analgesia and repeat imaging.
- Symptomatic, hypoxic, large or physiological compromise: insert a small-bore chest drain and admit.
- Needle aspiration may be considered in selected cases, but chest drain is often required.
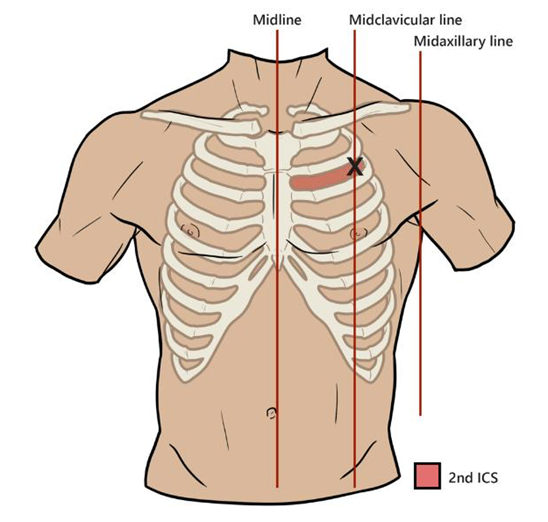
- Aspiration: Needle aspiration is a controlled procedure for a spontaneous pneumothorax when the patient is usually stable but symptomatic or has a larger pneumothorax. The aim is to aspirate air with a syringe/3-way tap and potentially avoid a chest drain. Site is 2nd ICS MCL, or 4th/5th ICS AAL or MAL, aspirate up to 2.5 L → repeat CXR.
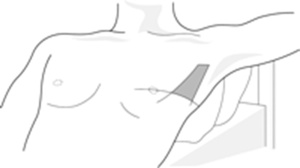
- Chest drain: Use a small-bore drain in most spontaneous pneumothoraces. Large-bore drains are usually reserved for trauma, haemothorax, very large air leak or specialist indications. Avoid routine suction initially; consider specialist advice if the lung fails to re-expand or there is persistent air leak. Indications: >2 cm and symptoms, failed aspiration, secondary PTX. Insert in safe triangle → monitor bubbling & swinging.
- When to involve thoracic surgery / consider VATS:
- Persistent air leak, often after 5–7 days depending on local policy and clinical context.
- Failure of lung re-expansion despite chest drainage.
- Recurrent ipsilateral pneumothorax.
- First contralateral pneumothorax.
- Bilateral spontaneous pneumothoraces.
- Spontaneous haemopneumothorax.
- High-risk occupation or activity, e.g. pilot, diver, remote worker.
- Patient preference after discussion of recurrence risk and treatment options.
- VATS procedure: VATS = video-assisted thoracoscopic surgery. Usually involves stapling/resection of visible blebs or bullae plus pleurodesis or pleural abrasion/pleurectomy to reduce recurrence. It is used mainly for recurrence prevention or persistent air leak, not as routine first-line treatment for every first pneumothorax.
- Discharge advice:
- Provide clear return precautions: worsening breathlessness, chest pain, syncope or collapse.
- Arrange follow-up chest imaging according to local pleural pathway.
- Avoid air travel until radiological resolution and specialist advice.
- Advise smoking cessation, as smoking significantly increases recurrence risk.
- Do not scuba dive after spontaneous pneumothorax unless definitively treated and cleared by a specialist diving medicine service.
🚨 Tension Pneumothorax:
- Emergency! Needle decompression → chest tube. Signs: severe distress, deviated trachea, distended neck veins, hypotension.
- Needle Decompression of Tension PTX Do not wait for imaging if the patient is unstable. Modern trauma teaching often uses 4th or 5th ICS, just anterior to the mid-axillary line. This is around the level of the nipple in males / inframammary fold area, but always count ribs if possible. Alternative is 2nd ICS mid-clavicular line, but failure rates can be higher because the chest wall is thicker and landmarking is often poor. Current sources describe both sites, with 4th/5th ICS anterior-to-mid-axillary or mid-axillary region increasingly preferred in trauma algorithms. Use a long large-bore cannula, often 14G/10–14G depending on local kit. Insert perpendicular to chest wall, just above the rib. Advance until air escapes / “hiss” is heard. Advance catheter over needle into pleural space. Remove needle, leave cannula in place.
Landmarks
⚠️ Complications
- 💨 Persistent air leak → may need thoracic surgery.
- 🦠 Infection (chest drain in situ).
- 🔁 Recurrence (esp. smokers, tall males).
📚 References

Cases - Pneumothorax (with size & management detail)
- Case 1 - Primary spontaneous 🌬️: A 22-year-old tall, slim man presents with sudden-onset left pleuritic chest pain and dyspnoea while at rest. No past medical history. Exam: hyper-resonance and absent breath sounds over the left chest. CXR: visible pleural line, 2 cm from the chest wall at the level of the hilum. Diagnosis: moderate primary spontaneous pneumothorax. Managed initially with needle aspiration; if unsuccessful, a chest drain would be placed.
- Case 2 - Secondary spontaneous 🫁: A 65-year-old man with GOLD stage 3 COPD presents with acute breathlessness and pleuritic pain. O₂ sats 85% on air. Exam: reduced breath sounds, hyper-resonance over right chest. CXR: right pneumothorax, 3 cm rim at the hilum. Diagnosis: large secondary pneumothorax. Managed with urgent chest drain insertion plus supplemental high-flow oxygen (if not hypercapnic).
- Case 3 - Traumatic / iatrogenic ⚡: A 34-year-old woman develops acute chest pain and breathlessness after insertion of a subclavian central line. Exam: tachypnoea, trachea central, reduced right-sided air entry. CXR: small right pneumothorax (<1 cm rim at hilum). Diagnosis: small iatrogenic pneumothorax. As she is stable and asymptomatic, managed with observation and repeat CXR in 24 hours.
Teaching Point 🩺: Size matters:
- Primary spontaneous PTX: <2 cm & stable → observe; ≥2 cm or breathless → aspirate (then chest drain if failed).
- Secondary spontaneous PTX: ≥2 cm or symptomatic → chest drain. 1–2 cm → attempt aspiration. <1 cm → admit, observe, and give O₂.
- Iatrogenic/traumatic PTX: often small and asymptomatic → observe; but if symptomatic or large, treat as above.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery