
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Metabolic alkalosis
Related Subjects: |Metabolic acidosis |Metabolic alkalosis |Arterial Blood gas analysis
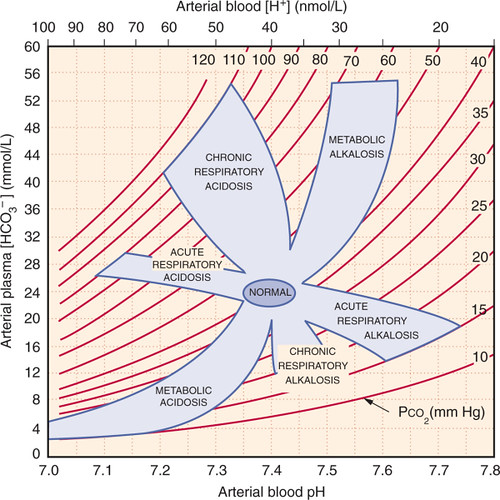
🌡️ Analysis of Blood Gas (Metabolic Alkalosis)
- 📉 pH > 7.45 (alkalosis)
- ⬆️ HCO₃⁻ increased (primary cause)
- PaCO₂ usually normal (unless compensated with hypoventilation)
- PaO₂ usually normal
- ⚡ Often associated with hypokalaemia
🔎 Aetiology
- Caused by either acid loss (vomiting, NG suction) or alkali gain (bicarbonate, milk-alkali syndrome).
📋 Causes and Management
| 🩺 Cause | 🤒 Clinical Features | 🔬 Diagnostic Tests | 💊 Management |
|---|---|---|---|
| 🤮 Vomiting / NG Suction | Loss of HCl → dehydration, postural hypotension | ABG: ↑pH, ↑HCO₃⁻
U&E: ↓Cl⁻, ↓K⁺ |
IV 0.9% NaCl + K⁺ replacement
Stop suction / treat vomiting |
| 💊 Diuretics (Loop / Thiazide) | Weakness, dizziness, dehydration | ABG: ↑pH, ↑HCO₃⁻
Electrolytes: ↓K⁺, ↓Cl⁻ |
Stop / adjust diuretic
IV saline + KCl supplements |
| 🧬 Hyperaldosteronism | HTN, muscle weakness, thirst, polyuria | ABG: ↑pH, ↑HCO₃⁻
Electrolytes: ↓K⁺, ↑Na⁺ Renin: ↓, Aldosterone: ↑ |
Treat cause (e.g., adrenal adenoma)
Spironolactone / eplerenone |
| 💉 Excess Bicarbonate | Confusion, paraesthesia, cramps, fluid overload | ABG: ↑pH, ↑HCO₃⁻
Electrolytes: ↑Na⁺, ↓K⁺ |
Stop bicarbonate
Treat underlying acidosis cause |
| ⚡ Hypokalaemia | Weakness, palpitations, arrhythmias (PVCs) | ECG: U waves, flat T waves
Serum: ↓K⁺ |
Potassium replacement (oral / IV)
Treat underlying cause |
| 💧 Contraction Alkalosis | Dehydration (dry mouth, low BP) | ABG: ↑pH, ↑HCO₃⁻
U&E: ↓Cl⁻, ↓K⁺ Urine Cl⁻: low |
IV 0.9% NaCl + KCl
Correct volume loss |
| 🥛 Milk-Alkali Syndrome | Nausea, vomiting, confusion, kidney stones | ABG: ↑pH
Electrolytes: ↑Ca²⁺, ↑HCO₃⁻ Creatinine ↑ |
Stop Ca²⁺ / antacids
IV fluids Severe hypercalcaemia → bisphosphonates |
📝 Key Clinical Pearls
- 🔄 Compensation is usually by hypoventilation (↑PaCO₂).
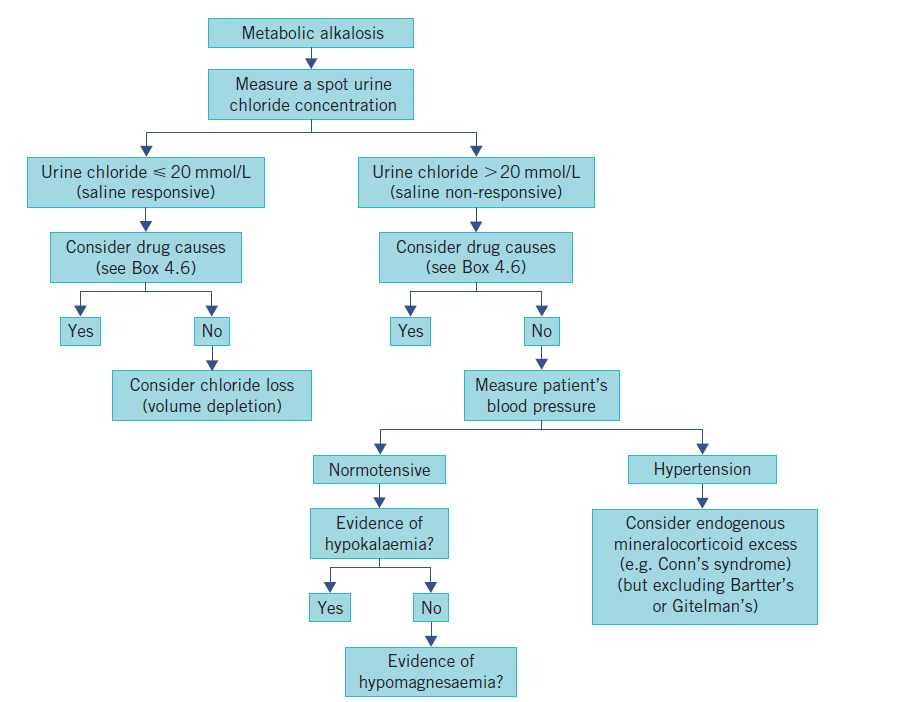
- 🧪 Urine chloride helps: low (<15 mmol/L) suggests vomiting/diuretics, high (>20 mmol/L) suggests mineralocorticoid excess.
- ⚠️ Hypokalaemia and hypochloraemia are hallmarks and must be corrected.
🩺 Case 1 - Vomiting-Induced Alkalosis
A 45-year-old woman presents with 5 days of persistent vomiting from severe gastritis. She is weak, dizzy, and hypotensive. Labs: pH 7.50, HCO₃⁻ 36 mmol/L, K⁺ 2.8 mmol/L, Cl⁻ low. Management: 💧 IV 0.9% saline and potassium replacement to correct volume and electrolyte deficits. Treat underlying cause of vomiting. Avoid: ❌ Continuing NG suction or antiemetics alone without fluid/electrolyte correction.
🩺 Case 2 - Diuretic-Induced Alkalosis
A 72-year-old man with chronic heart failure on furosemide presents with weakness and muscle cramps. Vitals stable. Labs: pH 7.48, HCO₃⁻ 34 mmol/L, K⁺ 3.0 mmol/L. Management: 💊 Review diuretic dose, replace potassium and magnesium, consider adding potassium-sparing diuretic (spironolactone, amiloride). Avoid: ❌ Escalating loop diuretic dose without electrolyte monitoring.
🩺 Case 3 - Post-Hypercapnic Alkalosis
A 65-year-old man with COPD on home oxygen is admitted with acute hypercapnic respiratory failure. After aggressive ventilation in ICU, his PaCO₂ normalises but labs now show pH 7.52, HCO₃⁻ 36 mmol/L, K⁺ 3.4 mmol/L. Management: 🏥 Careful weaning of ventilation, electrolyte correction (K⁺, Cl⁻), acetazolamide may be considered to promote renal bicarbonate excretion. Avoid: ❌ Over-ventilation leading to sudden CO₂ drop; avoid bicarbonate administration.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery