
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - NSTEMI
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Narrow complex tachycardia |ECG Ventricular fibrillation |ECG Regular Broad complex tachycardia |ECG Crib sheets
Typical ECG Findings in NSTEMI
Core Definition NSTEMI = myocardial infarction without persistent ST elevation on ECG but with troponin rise and ischaemic symptoms or ECG changes.
Key Message ECG is abnormal in ~80–90% of NSTEMI cases, but ~10–20% can have a completely normal or non-specific ECG → troponin is diagnostic. Changes are often dynamic → repeat ECG every 15–30 min if pain ongoing or high clinical suspicion.
Most Common & Typical ECG Changes
- ST-segment depression – most frequent and characteristic finding
- Horizontal or downsloping ≥0.5 mm (0.05 mV) in ≥2 contiguous leads
- Most common in lateral leads (I, aVL, V5–V6) or inferior leads (II, III, aVF)
- Can be widespread (anterior + lateral + inferior) in multivessel disease
- T-wave inversion – deep symmetric inversion (>2 mm) in ≥2 contiguous leads
- Common in anterior (V2–V4), lateral (I, aVL, V5–V6) or inferior leads
- Wellens' pattern (deeply inverted or biphasic T waves in V2–V3) indicates critical proximal LAD stenosis → urgent angiography
- Transient / brief ST elevation that resolves quickly before ECG capture
- Indicates unstable plaque with transient occlusion → still classified as NSTEMI if no persistent elevation
- Other supportive findings
- Hyperacute (tall, broad, peaked) T waves early in ischaemia
- Poor R-wave progression or loss of R waves (anterior infarction)
- New left bundle branch block (LBBB) with ischaemic symptoms → treat as STEMI equivalent
- Reciprocal ST depression opposite to subtle elevation
- Arrhythmias (sinus tachycardia, new atrial fibrillation, ventricular ectopics)
High-Risk ECG Patterns in NSTEMI
- Widespread ST depression in ≥3 leads + ST elevation in aVR → left main or triple-vessel disease
- Wellens' syndrome (deeply inverted or biphasic T waves V2–V3) → high-risk proximal LAD lesion
- Dynamic changes on serial ECGs (worsening depression, new T inversion)
- ST depression in multiple territories → multivessel ischaemia
Important Clinical Notes & Pitfalls
- Normal ECG does NOT exclude NSTEMI → always interpret with symptoms + troponin
- NSTEMI vs unstable angina → troponin elevation distinguishes (NSTEMI = troponin positive)
- Differentials for ST depression / T inversion: LVH with strain, digoxin effect, hypokalaemia, pulmonary embolism, takotsubo cardiomyopathy, myocarditis
- Always compare to previous ECGs if available
- Repeat ECG frequently during ongoing pain or if initial ECG non-diagnostic
Management Implications of ECG
- High-risk ECG (Wellens', widespread depression + aVR elevation, dynamic changes) → immediate invasive strategy (<2 hours to cath lab)
- Intermediate-risk → early invasive (<24 hours)
- Low-risk or non-specific changes → selective invasive or conservative approach
Clinical Pearl for Exams / OSCE / MCQ
- Most common ECG in NSTEMI → ST depression ± T-wave inversion in lateral or inferior leads
- Wellens' pattern or ST elevation in aVR + widespread depression → high-risk → urgent angiography
- Normal ECG does NOT rule out NSTEMI → rely on clinical picture + high-sensitivity troponin
- Always repeat ECG and compare serial changes in suspected ACS
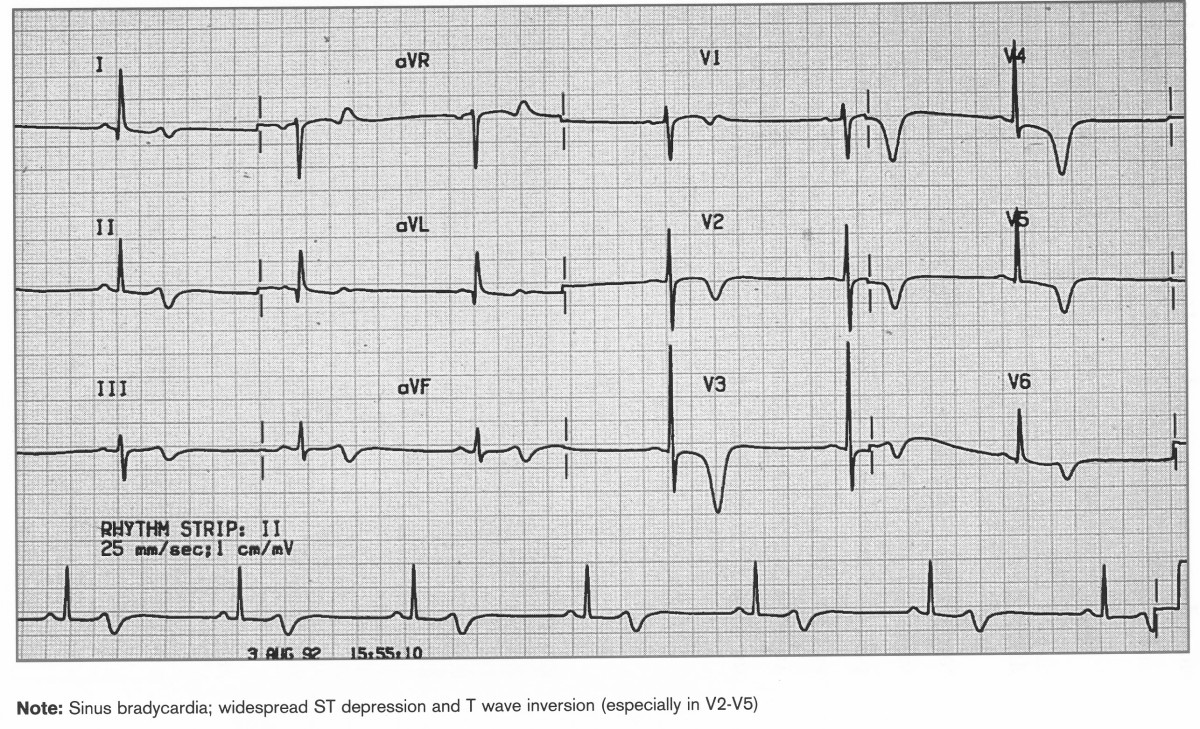
Chest pain at rest and ECG shows Sinus bradycardia, ST depression widespread, T wave inversion V2-5. Wellens Syndrome
Sources (2026)
- ESC Guidelines: Acute Coronary Syndromes (2023, minor 2025 updates)
- AHA/ACC NSTE-ACS Guideline (2022, reaffirmed 2025)
- NICE CG95 / NG185: Chest pain of recent onset (updated 2025)
- Life in the Fast Lane ECG Library (2026 updates)
- UpToDate: ECG in NSTEMI (2026)
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery