Related Subjects:
|Initial Trauma Assessment and Management
|Thoracic Trauma Assessment and Management
|Flail Chest Rib fractures
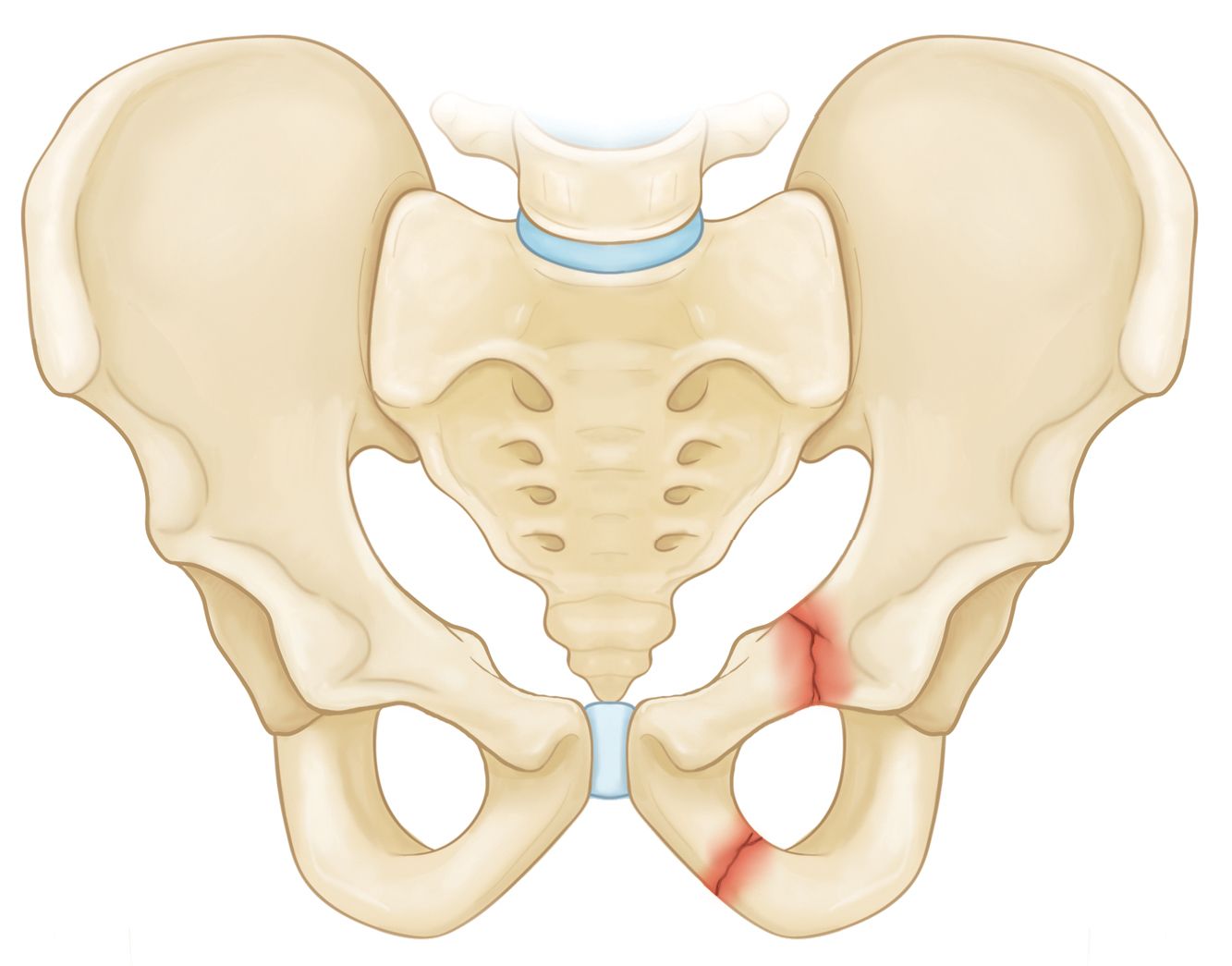
|Fractured Pubic Ramus
|Resuscitative Thoracotomy
|Haemorrhage control
|Traumatic Head/Brain Injury
|Traumatic Cardiac Arrest
|Abdominal trauma
|Tranexamic Acid
|Silver Trauma
|Cauda Equina
💡 Fractured Pubic Ramus: A common low-impact fragility fracture in the elderly, often following a fall from standing height.
⚠️ Up to 30% of patients never regain their prior level of independence, largely due to pain, immobility, and deconditioning.
📘 About
- Typically occurs after low-energy falls in frail older adults, particularly postmenopausal women with osteoporosis.
- Isolated pubic ramus fractures in younger patients are rare and usually due to high-energy trauma (e.g. RTCs, sports injuries).
⚙️ Aetiology
- Most common in elderly women in their mid-80s due to both reduced bone mineral density and increased fall risk.
- Risk factors: osteoporosis, sarcopenia, poor balance, polypharmacy, frailty, and anticoagulation (higher bleeding/haematoma risk).
🔍 Clinical Features
- History of a simple fall followed by groin, pubic, or inguinal pain.
- Pain worsens with weight-bearing, though some patients may still mobilise short distances.
- Examination may reveal groin or thigh bruising/haematoma, particularly in those on anticoagulants.
- Straight Leg Raise (SLR): ability to perform without pain makes a significant fracture very unlikely.
- Always consider medical precipitants for the fall (syncope, arrhythmia, infection, stroke, hypoglycaemia).
🧪 Investigations
- Bloods: FBC, U&E, calcium, ALP (bone turnover/osteoporosis), CRP/ESR if infection suspected.
- ECG: to rule out arrhythmia as cause of fall.
- Imaging: Pelvic X-ray is first-line. If negative but suspicion remains → CT pelvis (higher sensitivity).
🩺 Management
- Core aims: analgesia, early mobilisation, prevention of complications, and secondary prevention of fractures/falls.
- Analgesia: stepwise with paracetamol → weak opioids if needed. NSAIDs rarely first-line in frail elderly due to GI/renal risks.
- Mobilisation: encourage physiotherapy-led mobilisation as soon as tolerated to prevent deconditioning, pneumonia, and thromboembolism.
- VTE prophylaxis: LMWH unless contraindicated (consider renal function, bleeding risk).
- Bone health optimisation: DEXA scan, vitamin D and calcium supplementation, bisphosphonates or other antiresorptive agents as appropriate.
- Falls risk assessment: OT input, home environment safety review, medication rationalisation, vision/hearing assessment.
📖 References
- British Orthopaedic Association (BOA): Guidance on Fragility Fractures.
- NICE NG56: Multimorbidity and Falls in Older People.
- Royal Osteoporosis Society – Fragility Fractures.