
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Charcot Foot Syndrome (CFS)
🦶 Charcot Foot Syndrome (CFS) is one of the most devastating complications affecting patients with diabetes and peripheral neuropathy.
📖 About
- Neuropathic joint → loss of sensation, so damage may go unnoticed.
- Progressive bone and joint deformity → destructive arthritis 🦴.
- Associated with a mean reduction in life expectancy of ~14 years ⏳.
⚠️ Causes (any sensory neuropathy)
- Diabetic neuropathy (most common) 🍬
- Tabes dorsalis (syphilis)
- Syringomyelia (upper limbs)
- Alcoholic neuropathy 🍷
- Cerebral palsy with sensory loss
- Leprosy 🦠
- Congenital insensitivity to pain
⚙️ Aetiology
- Neurotraumatic theory: Repetitive trauma + loss of pain/proprioception → bony destruction.
- Neurovascular theory: Autonomic hyperaemia → osteopenia + trauma → joint collapse.
- Intrinsic muscle imbalance → eccentric loading → microfractures, laxity, deformity.
🔎 Clinical Features
- Numbness, redness, swelling (pain only in ~50%).
- Injuries, fractures, deformity 🦴.
- Peripheral neuropathy (fails 10 g monofilament test).
- Assess arterial perfusion: pulses (palpation/Doppler) 💓.
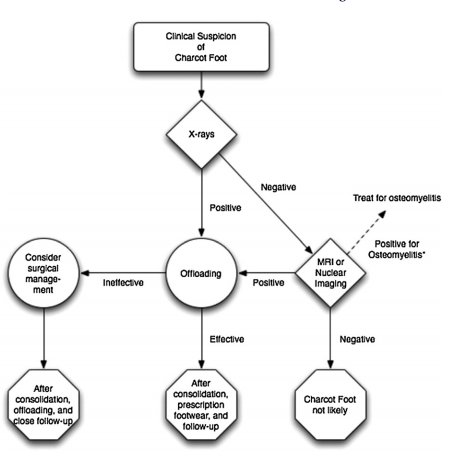
🧪 Investigations
If acute Charcot arthropathy is suspected → arrange weight-bearing X-ray. If X-ray is normal but suspicion remains → MRI 🖥️.
- Bloods: FBC, U&E, LFT, urate, glucose, HbA1c, CRP (raised CRP → ?osteomyelitis).
- Blood cultures if infection suspected.
- Infrared dermal thermography: >2.0°C difference vs contralateral side 🌡️.
- Plain weight-bearing radiographs.
- MRI: stress fractures, fragmentation, subluxation/dislocation, osteopenia, osteolysis.
- Indium-111 leukocyte scan for osteomyelitis if unclear.
🔍 Differential Diagnosis
- Osteomyelitis 🦠
- Acute gout 🦶🔥
- DVT 🩸
- Deep abscess
- Inflammatory arthritis
🖼️ Imaging
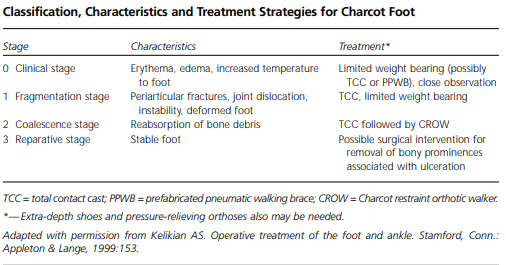
🩺 Management
- Urgent referral: Within 1 working day → multidisciplinary foot service (NICE NG19).
- Immediate: Non-weight-bearing + immobilisation (total contact cast) until resolution.
- Step-down: Gradual partial weight bearing as advised.
- Moderate deformity: Custom footwear + offloading orthotics 👟.
- Severe deformity: CROW boot; consider surgical referral 🛠️.
- Psychological support + physiotherapy for strengthening 💪.
- 3-monthly reviews to monitor for reactivation 🔄.
💡 Exam Tip: In suspected acute Charcot foot, the key is urgent referral + non-weight-bearing. Confusing it with cellulitis or osteomyelitis is a classic exam trap ⚡.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery