⏱️ 0–5 minutes: Immediate safety + ABC
- Call for help early: crash team, resus team, ICU outreach, anaesthetics or senior medical help depending on setting.
- Check for an individualised epilepsy emergency management plan if immediately available, and follow it while continuing ABC resuscitation.
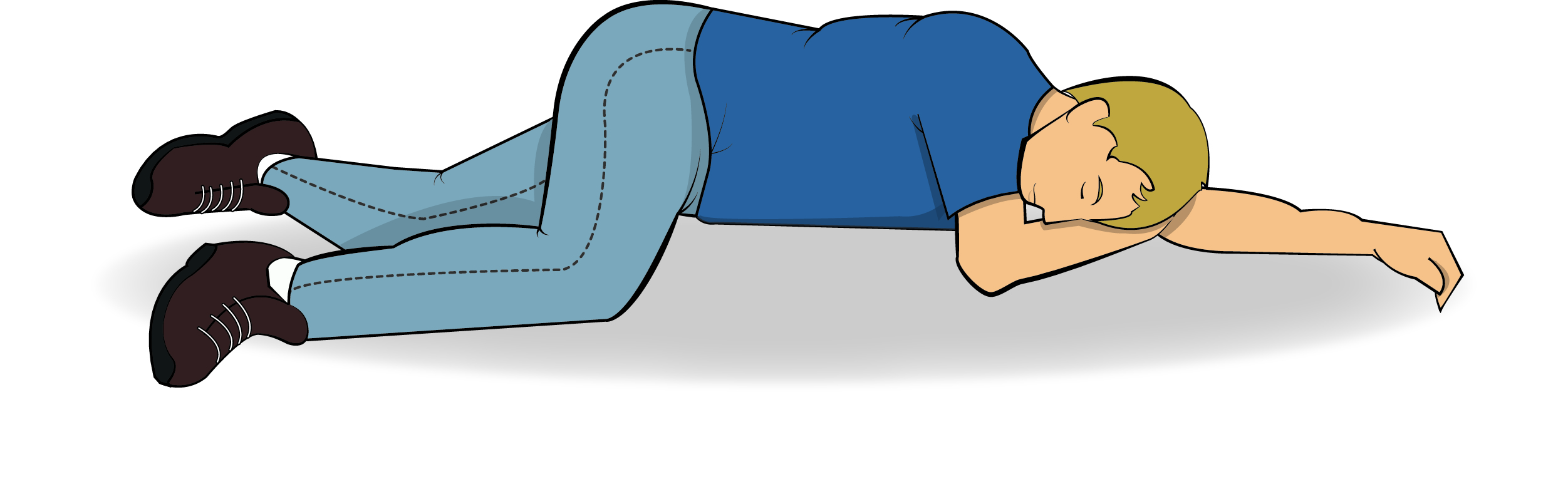
- Protect from injury; do not restrain; remove hazards; loosen tight clothing around the neck; place in the recovery position when feasible.
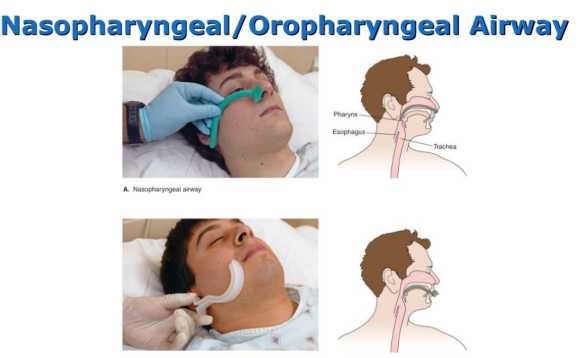
- Airway: suction, jaw thrust, consider airway adjuncts if tolerated, and prepare for bag-mask ventilation.
- Breathing: monitor SpO₂, support ventilation if needed, and give high-flow oxygen if hypoxaemic, cyanosed, peri-arrest, or if saturations cannot be reliably measured during ongoing convulsions. Once stable, titrate oxygen to 94–98%, or 88–92% if at risk of hypercapnic respiratory failure.
- Circulation: ECG monitoring, blood pressure, pulse, IV access x2 if possible.
- Glucose: check capillary glucose immediately. If low, treat without delay.
- Hypoglycaemia treatment - typical adult:
- Give IV glucose 10%, for example 100–200 mL, and recheck glucose.
- If no IV access, give IM glucagon 1 mg.
- Consider IV Pabrinex / thiamine before or alongside glucose if alcohol misuse, malnutrition or Wernicke risk is suspected, according to local protocol.
- Bloods, but do not delay treatment: FBC, U&E, LFT, calcium, magnesium, glucose, CRP, CK, VBG/ABG ± lactate, toxicology/ethanol if indicated, pregnancy test where relevant, and antiseizure medication levels if applicable.
- Check temperature; start cooling measures if hyperthermic.
- Treat obvious triggers early, such as sepsis, electrolyte disturbance, drug toxicity, withdrawal, meningitis or encephalitis.
⏱️ 5–10 minutes: First-line benzodiazepine
- Check what has already been given by carers, ambulance staff, care home staff or family. Include pre-hospital buccal midazolam or rectal diazepam in the maximum of 2 benzodiazepine doses.
- Give one benzodiazepine dose promptly via the fastest appropriate route.
- Community or no IV access: give buccal midazolam, or rectal diazepam if midazolam is unavailable or unsuitable.
- Hospital with IV access and resuscitation facilities: give lorazepam 4 mg IV slowly. Monitor respiration closely.
- If no IV access in hospital: use buccal, intramuscular or intranasal midazolam according to local protocol.
- Airway warning: benzodiazepines can cause hypoventilation, especially after repeated doses. Be ready to use airway manoeuvres and bag-mask ventilation.
- Pregnancy with suspected eclampsia: give magnesium sulfate 4 g IV loading dose, then infusion according to obstetric protocol, and call obstetrics, anaesthetics and senior help urgently.
⏱️ 10–20 minutes: If ongoing, repeat benzodiazepine once
- If convulsions persist after the initial dose, repeat one further benzodiazepine dose after approximately 5–10 minutes.
- Do not exceed 2 benzodiazepine doses unless under senior specialist direction, because seizure-control benefit falls while respiratory depression risk rises.
- Continue continuous monitoring and prepare second-line IV antiseizure loading treatment.
- Escalate early to anaesthetics/ICU if seizures continue, airway risk is rising, or second-line treatment is being prepared.
⏱️ 20–30 minutes: Second-line IV antiseizure loading - choose one
- Start a loading dose promptly if seizures continue after two benzodiazepine doses. Choice depends on comorbidity, pregnancy potential, interactions, liver disease, cardiac disease and local availability.
- Levetiracetam: 60 mg/kg IV, maximum 4.5 g, over 10–15 minutes.
- Often practical because it has fewer drug interactions and is relatively easy to administer.
- It may still be used in people already prescribed levetiracetam, but check local or specialist advice.
- Phenytoin: 20 mg/kg IV, maximum 2 g, at no more than 50 mg/min.
- Use ECG and blood pressure monitoring.
- Avoid or use extreme caution in severe conduction disease, bradyarrhythmia or significant cardiac disease.
- Watch for extravasation injury and drug interactions.
- Sodium valproate: 40 mg/kg IV, maximum 3 g, over about 10 minutes.
- Avoid in pregnancy.
- Generally avoid in women and girls of childbearing potential unless specialist advice confirms that no suitable alternative is appropriate.
- Follow MHRA valproate safety measures.
- Avoid in significant liver disease and suspected mitochondrial disorders.
- Escalate early: alert ICU/HDU, anaesthetics and neurology when giving second-line therapy.
⏱️ ≥30 minutes: Refractory status epilepticus - expert guidance, phenobarbital and/or ICU anaesthesia
- If seizures persist after second-line treatment, seek urgent neurology, ICU and anaesthetic guidance.
- Consider phenobarbital or general anaesthesia under expert guidance.
- If general anaesthesia is used: secure airway, intubate, ventilate and start an anaesthetic infusion according to ICU protocol.
- Common ICU infusions include propofol or midazolam; monitor for hypotension and complications. Prolonged high-dose propofol carries risk of propofol infusion syndrome.
- Use continuous EEG if available, because convulsive status can evolve into non-convulsive status epilepticus after motor activity stops.
- Actively correct physiology: oxygenation, ventilation, temperature, glucose, sodium, calcium, magnesium, acidosis and renal function.
Beyond refractory status: Specialist strategies
- Ketamine may be considered in specialist settings, particularly later when NMDA-mediated excitation is more important.
- Barbiturate anaesthesia, for example thiopental or pentobarbital, may be used in specialist ICUs.
- Consider immune, infective and structural causes early, including autoimmune encephalitis, HSV encephalitis, meningitis, stroke, haemorrhage and tumour.
- Start empirical antimicrobial or antiviral treatment promptly if infection or encephalitis is suspected; do not wait for LP if this would cause delay.
🧠 Post-stabilisation - once safe
- Confirm seizure termination clinically and with EEG if there is any doubt. Persistent coma, fluctuating awareness or subtle twitching may indicate non-convulsive status epilepticus.
- Neuroimaging: CT head urgently if first seizure, focal neurological deficit, immunosuppression, head injury, anticoagulation, persistent reduced GCS, or suspicion of haemorrhage, stroke, tumour or raised intracranial pressure.
- Lumbar puncture: perform if meningitis or encephalitis is suspected, after imaging if raised intracranial pressure risk is present.
- Empirical therapy: if HSV encephalitis is suspected, start IV aciclovir immediately; do not wait for LP if delayed.
- Antiseizure medication plan: optimise long-term treatment, check adherence, interactions and levels where relevant, and involve neurology or the epilepsy team.
- Emergency plan: after recovery, agree or update an individualised emergency management plan if prolonged seizures or status epilepticus may recur.
- Driving and safety: give appropriate advice about driving restrictions, bathing, swimming, heights, machinery and occupational risks.
⚠️ Common causes and triggers
- Known epilepsy: missed antiseizure medication, sleep deprivation, alcohol use or withdrawal, infection, interacting drugs, vomiting, malabsorption or recent medication changes.
- New-onset seizures: stroke, intracranial haemorrhage, tumour, meningitis, encephalitis, head injury, hyponatraemia, hypocalcaemia, hypoglycaemia, toxins, drugs or alcohol withdrawal.
- Mimics: psychogenic non-epileptic seizures, syncope, hypoglycaemia, dystonia, rigors and drug reactions.
🚨 Complications to anticipate
- Airway and respiratory: aspiration, hypoventilation after benzodiazepines, airway obstruction, hypoxia and respiratory failure.
- Systemic: hyperthermia, lactic acidosis, rhabdomyolysis, acute kidney injury, electrolyte disturbance and arrhythmias.
- Neurological: hypoxic brain injury, cerebral oedema and non-convulsive status epilepticus.
- Inpatient risks: pressure injury, aspiration pneumonia and VTE from immobility. Start VTE prophylaxis when safe.
|