
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Normal Pressure Hydrocephalus
Related Subjects: |Dementias |Abbreviated Mental Test Score (AMTS) |Alzheimer disease |Dementia with Lewy bodies |Frontotemporal dementia |Corticobasal degeneration |Creutzfeldt Jakob disease |Vascular Dementia |Primary progressive aphasia |Anti Dementia Drugs |AIDS Dementia Complex |Normal Pressure Hydrocephalus |Acetylcholinesterase inhibitors |Mental Capacity Act 2005 |Behavioural and Psychological Symptoms of Dementia
Note: The diagnosis of Normal Pressure Hydrocephalus (NPH) remains controversial ⚖️. Many older adults have gait disturbance, cognitive decline, and ventriculomegaly due to atrophy rather than true NPH. The challenge is identifying those who will genuinely benefit from shunting, as complications are significant.
🌙 About
- NPH is a potentially reversible cause of dementia caused by abnormal CSF accumulation in the ventricles without raised intracranial pressure.
- Classically affects those >60 years old 👴 and was first described by Salomon Hakim in 1965.
- Pathophysiology: Thought to be due to impaired CSF absorption at arachnoid villi → gradual ventricular dilation → compression of periventricular white matter tracts.
⚠️ Causes
- Idiopathic: Majority of cases.
- Secondary: Post-traumatic brain injury, meningitis, subarachnoid haemorrhage (SAH), or tumours obstructing CSF pathways.
🔬 Aetiology
- Disruption of white matter tracts → gait + bladder dysfunction.
- Cortical compression → cognitive slowing and apathy.
- Not fully understood; research into CSF dynamics and glymphatic system is ongoing.
🧩 Clinical Features – Hakim’s Triad
- 🚶♂️ Gait disturbance: “Magnetic gait” (feet stuck to floor), shuffling, difficulty initiating steps.
- 💧 Urinary incontinence: Urgency, frequency, progressing to frank incontinence.
- 🧠 Cognitive decline: Apathy, slowed thought, impaired planning; memory loss less pronounced early on compared to Alzheimer’s.
💡 Mnemonic: "Wet, Wobbly, Wacky" (incontinence, gait, cognition)
🩺 Differential Diagnosis
- Alzheimer’s disease & vascular dementia 🧠
- Parkinson’s disease & atypical parkinsonism 🤚
- Spinal stenosis (gait mimic) 🦴
- Chronic subdural haematoma (exclude with CT/MRI) 💉
📊 Investigations
- Lumbar puncture: Normal opening pressure; large-volume tap (30–40 mL) → transient improvement in gait/cognition suggests shunt responsiveness.
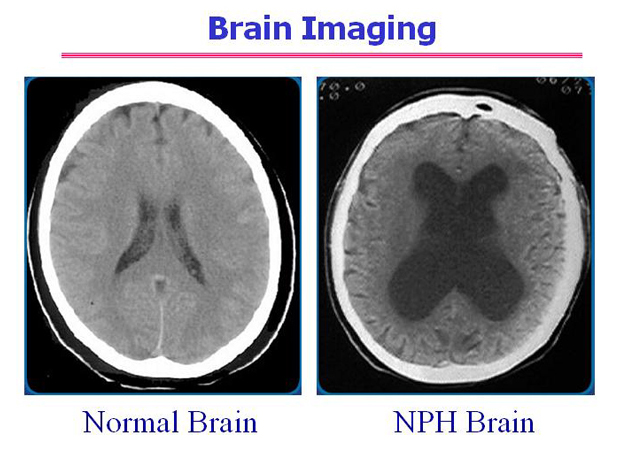
- CT: Ventriculomegaly out of proportion to atrophy (Evans’ index >0.3).
- MRI: Periventricular hyperintensity due to transependymal CSF flow.
- Gait assessment: Before & after LP to assess reversibility.
🖼️ CT scan of NPH
💊 Management
- Pre-shunt testing: LP or external lumbar drainage to select responders.
- Ventriculoperitoneal (VP) shunt: Diverts CSF → peritoneum.
- 🎯 Improvement: 20–90% improve, esp. gait first.
- ⚠️ Complications: infection, bleeding, overdrainage → subdural haematoma.
- Adjustable shunts allow fine-tuning of drainage pressure.
- Conservative: In frail/non-candidates → fall prevention, continence support, therapy.
- Rehabilitation: PT/OT for gait training & ADLs even if shunt is not performed.
📈 Prognosis
- Best outcome if diagnosed early & shunted after positive LP response.
- Gait improves most reliably 🚶♂️, cognition & bladder symptoms less predictable.
- Untreated → progressive disability, dementia, and falls risk.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery