
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Oesophagus
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
🦴 Anatomy of the Oesophagus
The oesophagus is a muscular tube (~25 cm long) that transports swallowed material from the pharynx to the stomach. It begins at the pharyngoesophageal junction (lower border of the cricoid cartilage, C6) and ends at the gastro-oesophageal junction (GOJ) where squamous mucosa transitions to columnar gastric mucosa (the Z-line). Beyond being a “pipe”, it is a finely coordinated motor organ: it initiates peristalsis, generates a barrier against reflux, and coordinates sphincter relaxation to allow safe bolus transit. 🌊
📍 Position, Course, and Key Levels
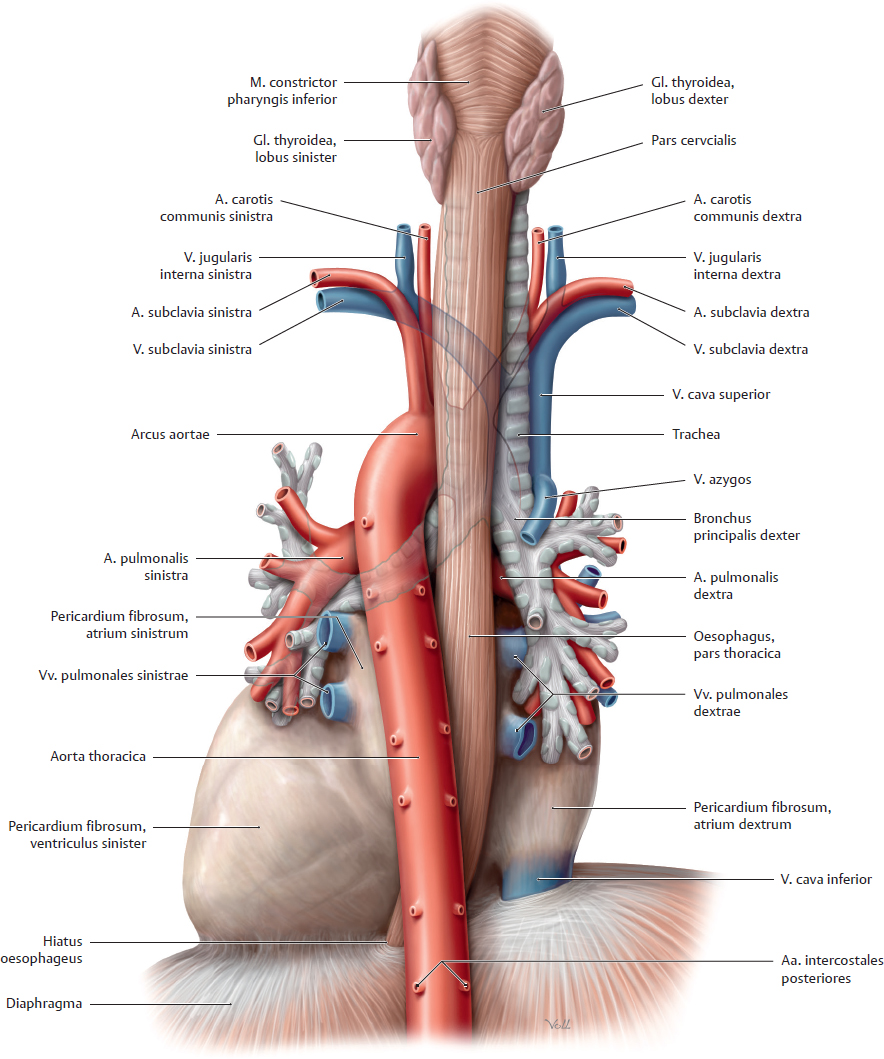
- General course: Descends in the neck and posterior mediastinum, lying posterior to the trachea and anterior to the vertebral column, then passes through the diaphragm to join the stomach.
- Diaphragmatic passage: traverses the oesophageal hiatus at T10.
Mnemonic: “I 8 10 Eggs At 12” → IVC T8, Oesophagus T10, Aorta T12 - Left atrial relation: In the thorax, the oesophagus lies close behind the left atrium (important for TOE/TEE and for symptoms from LA enlargement).
- Clinical landmarks for endoscopy: distances are often measured from the incisors to locate lesions/strictures.
🏷️ Anatomical Divisions
- Cervical oesophagus: Begins at C6 → thoracic inlet. Closely related to the trachea anteriorly and vertebral bodies posteriorly.
- Thoracic oesophagus: Thoracic inlet → diaphragm. Traverses the posterior mediastinum; intimately related to the aortic arch and left main bronchus (sites of narrowing).
- Abdominal oesophagus: Short (~1–2 cm) segment below the diaphragm → GOJ and gastric cardia.
🧭 Relations (High-yield Anatomy)
- Anterior: trachea (upper), then left main bronchus, then pericardium/left atrium (mid-lower thorax).
- Posterior: vertebral column; thoracic duct; azygos system (regional).
- Right side: azygos vein, mediastinal pleura (regional).
- Left side: aortic arch/descending thoracic aorta and mediastinal pleura (regional).
- At the hiatus: diaphragmatic crura form an external “pinch-cock” effect that contributes to the anti-reflux barrier.
🧩 Layers of the Oesophageal Wall (Structure ↔ Function)
- Mucosa: Non-keratinised stratified squamous epithelium - abrasion-resistant for bolus transit.
Clinical: chronic reflux can drive metaplasia to columnar epithelium (Barrett’s). - Submucosa: elastic tissue with mucous glands → lubrication and protection; contains the submucosal (Meissner) plexus.
- Muscularis externa: two coordinated layers generate peristalsis:
- Inner circular layer: constricts behind the bolus.
- Outer longitudinal layer: shortens the segment ahead of the bolus, reducing resistance.
- Muscle type gradient: upper 1/3 skeletal, middle 1/3 mixed, lower 1/3 smooth - the anatomical basis for the transition from voluntary to involuntary propulsion.
- Adventitia: outer connective tissue anchoring the oesophagus to surrounding structures (note: unlike the stomach, much of the oesophagus is not fully peritonealised).
🚪 Sphincters & the Anti-reflux Barrier
The oesophagus has two functional sphincters: the upper oesophageal sphincter (UES) prevents air entry and aspiration, while the lower oesophageal sphincter (LES) and diaphragmatic hiatus create a high-pressure zone that prevents reflux. Importantly, the LES is not a discrete “ring” like a valve; it is a physiological high-pressure segment shaped by smooth muscle tone, the diaphragm, and the angle of the GOJ.
- UES: largely the cricopharyngeus muscle.
- At rest: tonically contracted → prevents aerophagia and reflux into pharynx.
- During swallow: relaxes and opens in synchrony with pharyngeal contraction.
- LES / GOJ complex:
- Basal tone prevents gastric content reflux.
- Relaxation is triggered by swallow-induced inhibitory neurons (NO/VIP mediated).
- Additional components: diaphragmatic crura, the angle of His, and the intra-abdominal oesophageal segment (positive pressure zone).
- Failure contributes to GORD/GERD, oesophagitis, stricture, and Barrett’s.
🩸 Blood Supply, Venous Drainage, Lymphatics & Innervation
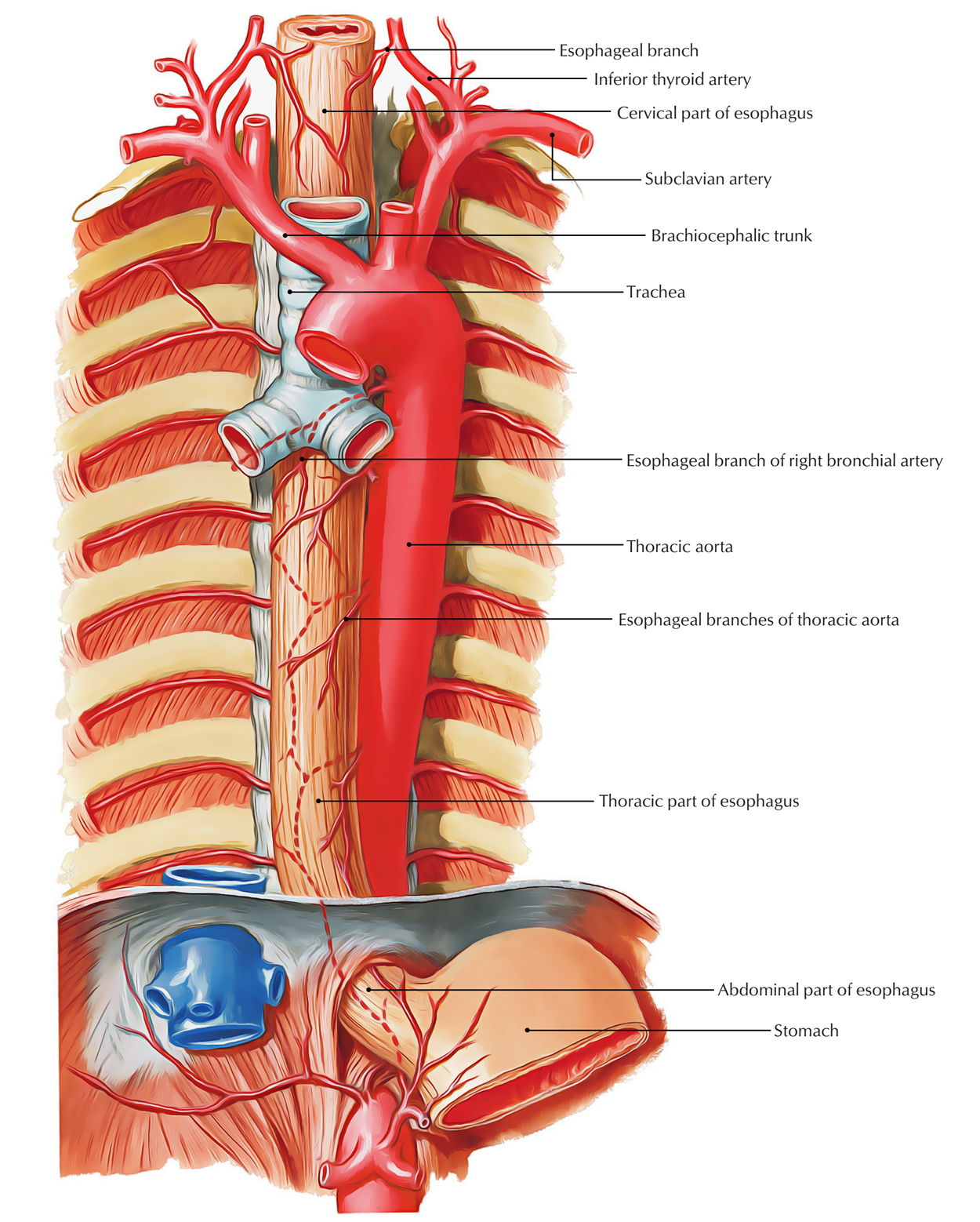
- Arterial supply (segmental):
- Cervical: inferior thyroid artery branches.
- Thoracic: oesophageal branches from thoracic aorta ± bronchial arteries.
- Abdominal: left gastric artery ± inferior phrenic branches.
- Venous drainage:
- Cervical: inferior thyroid veins.
- Thoracic: azygos/hemiazygos system.
- Abdominal: left gastric vein → portal vein.
- Key clinical concept: the distal oesophagus is a site of porto-systemic anastomosis → oesophageal varices in portal hypertension.
- Lymphatics: follow segmental pattern (cervical → deep cervical nodes; thoracic → posterior mediastinal; distal → left gastric/celiac).
Clinical: this contributes to early lymphatic spread of oesophageal cancer and “skip” metastases. - Innervation:
- Vagus nerve: major parasympathetic control of peristalsis and sphincter function.
- Enteric nervous system: myenteric (Auerbach) plexus coordinates smooth muscle contraction/relaxation.
- Sympathetic: modulates blood flow and can influence motility (stress-related symptom exacerbation).
- Pain referral: visceral afferents can refer discomfort retrosternally (reflux/oesophagitis can mimic cardiac pain).
⚙️ Physiology of Swallowing (Deglutition)
Swallowing is a coordinated sequence that protects the airway while propelling a bolus efficiently into the stomach. It has oral (voluntary), pharyngeal (reflex), and oesophageal (reflex) phases. The “swallowing centre” in the medulla coordinates cranial nerves and triggers a wave of peristalsis while transiently inhibiting respiration to prevent aspiration.
- Oral phase (voluntary): tongue propels bolus posteriorly → triggers swallow reflex.
- Pharyngeal phase (reflex):
- Soft palate elevates to close nasopharynx.
- Larynx elevates and vocal cords adduct; epiglottis helps protect the airway.
- UES relaxes and opens; pharyngeal constrictors push bolus into oesophagus.
- Oesophageal phase (reflex): coordinated peristaltic wave + LES relaxation to allow entry into stomach.
🌊 Peristalsis & Motility (How the bolus moves)
- Primary peristalsis: initiated by swallowing; propagates from UES to LES.
- Secondary peristalsis: triggered by oesophageal distension/residual bolus; important for “clearing” refluxed acid.
- Mechanics: circular muscle contraction behind bolus + longitudinal shortening ahead reduces lumen resistance.
- Neurotransmitters:
- Excitatory: acetylcholine/substance P → contraction.
- Inhibitory: nitric oxide (NO) and VIP → relaxation (critical for LES relaxation).
🛡️ Mucosal Protection & Reflux Defence
The oesophagus is not built to tolerate acid long-term, so its defence relies on barrier mechanisms (LES + diaphragm + anatomy) and clearance mechanisms (peristalsis + saliva). When these fail or acid exposure is prolonged, inflammation and metaplastic change can occur.
- Barrier: LES tone, diaphragmatic crura, intra-abdominal oesophagus, angle of His.
- Clearance: secondary peristalsis + saliva (bicarbonate) neutralisation.
- Exposure factors: delayed gastric emptying, obesity, pregnancy, hiatus hernia, medications reducing LES tone.
📊 Physiological Narrowings (Constrictions) - High yield
These are common sites for food bolus impaction, pill injury, corrosive burns, and endoscopic “hold-ups”. They are also important radiological landmarks.
- 📌 Pharyngoesophageal junction (C6, cricoid/UES)
- 📌 Aortic arch impression (around T4)
- 📌 Left main bronchus impression (around T5/6)
- 📌 Diaphragmatic hiatus (T10)
🧪 Function at the Gastro-oesophageal Junction (Z-line & metaplasia)
- Z-line: transition from squamous oesophageal epithelium to columnar gastric epithelium.
- Barrett’s oesophagus: intestinal metaplasia from chronic reflux; increases oesophageal adenocarcinoma risk (clinical surveillance context).
- Strictures: chronic inflammation and scarring can narrow lumen → progressive dysphagia (solids then liquids).
🩺 Clinical Correlations (Anatomy + Physiology → Symptoms)
- Dysphagia:
- Oropharyngeal (transfer problem) suggests neurological disease, structural pharyngeal pathology, aspiration risk.
- Oesophageal (transport problem) suggests obstruction (stricture/cancer) or motility disorder (achalasia, spasm).
- Reflux (GORD/GERD): heartburn/regurgitation; complications include oesophagitis, strictures, Barrett’s.
- Achalasia physiology (core concept): failure of inhibitory neurons → impaired LES relaxation + absent peristalsis → dysphagia to solids and liquids, regurgitation (manometry diagnosis).
- Varices: portal hypertension → dilated submucosal veins in distal oesophagus → massive upper GI bleeding risk.
- TOE/TEE: oesophagus is a key “acoustic window” to the left atrium/mitral valve because of close posterior relation.
- Oesophageal cancer: often presents with progressive dysphagia and weight loss; common at physiological narrowings and at GOJ.
📝 Summary
The oesophagus is a 25 cm muscular conduit from C6 to the stomach that combines abrasion-resistant squamous mucosa with a sophisticated motility system. Swallowing triggers primary peristalsis and coordinated sphincter relaxation, while secondary peristalsis and saliva help clear refluxed acid. The anti-reflux barrier depends on LES tone plus diaphragmatic and anatomical supports at the GOJ; failure leads to GORD and complications such as strictures and Barrett’s. Clinically, dysphagia localises disease (transfer vs transport), and the distal oesophagus is a key porto-systemic site explaining variceal bleeding in portal hypertension.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery