Related Subjects: Small Bowel Obstruction
|Colonic (Large bowel) Obstruction
|Caecal Volvulus
|Small Bowel Ischemia
|Hartmann's procedure
|Sigmoid Volvulus
|Acute Colonic Pseudo-obstruction
| Metabolic acidosis
| Lactic acidosis
|Rectal Prolapse
|Anal Cancer
|Anal Fissure
|Pilonidal Abscess (sinus)
|Haemorrhoids (Piles)
|Hartmann's procedure
🚨 Small Bowel Obstruction (SBO) is a surgical emergency. It most often arises from adhesions after previous laparotomy, but can also result from hernia, Crohn’s disease, or intussusception.
⚠️ Diagnosis is often delayed, leading to perforation, sepsis, and high mortality if not recognised early.
| 🩺 Initial Management of SBO |
|---|
- ABC, Oxygen, IV fluids 💧: 3–4 L resuscitation unless in CCF.
- Bloods 🧪: FBC, U&E, CRP; correct K⁺/Mg²⁺/Ca²⁺ abnormalities.
- NG tube ➡️ decompression: If vomiting, prevents aspiration.
- Urinary catheter: For accurate fluid balance; replace NG/urinary losses.
- Analgesia: Opiates with caution; cyclizine for nausea (avoid metoclopramide).
- Monitor bloods: Lactate ↑, metabolic acidosis, rising WCC → suspect ischaemia.
- Imaging: Erect AXR, supine AXR, erect CXR (free air → perforation).
- CT abdomen: Gold standard for transition point and cause of obstruction.
- Functional obstruction: Stop causative meds (opiates, anticholinergics), correct electrolytes.
- Sepsis 🔥: Treat aggressively, consider HDU/ICU if unstable.
- Mechanical obstruction: Surgery if strangulated/peritonitic.
|
📖 About
- SBO is one of the most common causes of acute surgical admission.
- Can present as total (complete) or subtotal (partial) obstruction.
- Mortality is driven by ischaemia and perforation → rapid recognition is vital.
🧬 Aetiology
- Pathophysiology: Obstruction → proximal bowel dilatation, bacterial overgrowth, fluid sequestration → perforation risk at maximum diameter site (usually caecum).
- Strangulation impairs blood supply → necrosis and sepsis.
🔎 Causes
- Luminal: Tumour, gallstone ileus, foreign body, bezoar, faecal impaction.
- Mural: Crohn’s stricture, neoplasm, radiation stricture, ischaemia, pseudo-obstruction.
- Extramural: Adhesions (most common in UK), hernias, volvulus, intussusception, peritoneal TB, pelvic/ovarian malignancy.
👩⚕️ Clinical Features
- Symptoms: Colicky central abdominal pain, bilious vomiting, abdominal distension, constipation/obstipation.
- Signs: Dehydration, tachycardia, tender/distended abdomen, high-pitched "tinkling" bowel sounds.
Late → peritonitis, shock, sepsis.
🧪 Investigations
- Bloods: FBC, U&E, lactate, amylase, CRP.
Raised lactate → ischaemia/strangulation.
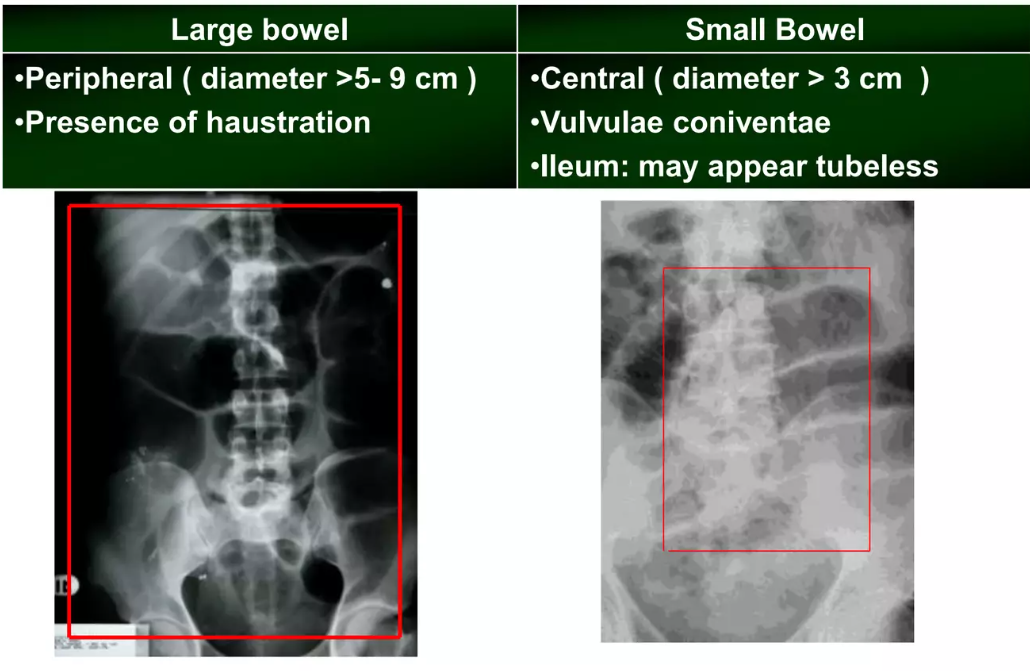
- AXR: Dilated central loops, valvulae conniventes across lumen, fluid levels.
- CXR: Free air under diaphragm = perforation.
- CT abdomen: Transition point, closed loop obstruction, evidence of strangulation.
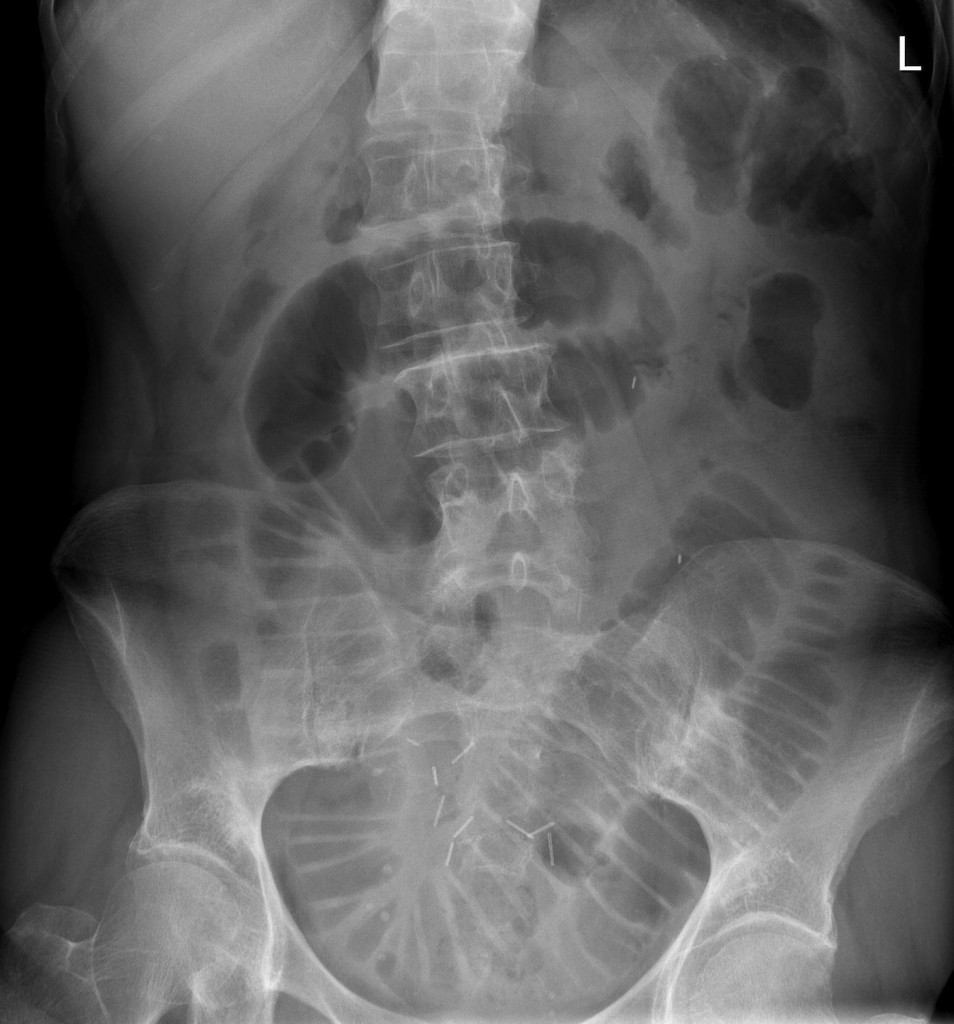
📷 Example AXR
The valvulae conniventes are clearly demonstrated. Central distended small bowel loops with visible old surgical staples. Cause: adhesions.
📊 Comparison: Small vs Large Bowel Obstruction
| Feature | Small Bowel | Large Bowel |
|---|
| Abdominal Pain | Early, colicky, central | Dull, less colicky |
| Vomiting | Early bilious, late faeculent | Occurs later |
| Constipation | Late feature | Early, may pass diarrhoea if partial |
| Distension | Less if high obstruction; marked if distal | Marked, esp. sigmoid/caecal volvulus |
| Bowel Sounds | High-pitched "tinkling" | Often reduced or absent late |
| AXR | Central dilated loops, valvulae conniventes across bowel | Peripheral dilatation, haustra not spanning full lumen |
| Common Causes | Adhesions, hernia, Crohn’s, volvulus | Colorectal cancer, sigmoid volvulus, diverticular disease |
💊 Management
- Resuscitation: IV fluids, electrolyte correction, catheterisation.
- Decompression: NG tube on free drainage.
- Antibiotics: Broad-spectrum (gram-negative + anaerobes) if perforation or sepsis suspected.
- Surgical intervention: Emergency laparotomy for peritonitis, perforation, or ischaemia.
Adhesiolysis or resection depending on cause.
- Medical: Conservative trial if partial obstruction (esp. adhesions) with close monitoring.
- Palliative: For advanced malignancy or poor surgical candidates.
📚 References
