
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
CT Basics for Stroke
Related Subjects: |Acute Stroke Assessment (ROSIER&NIHSS) |Atrial Fibrillation |Atrial Myxoma |Causes of Stroke |Ischaemic Stroke |Cancer and Stroke |Cardioembolic stroke |CT Basics for Stroke |Endocarditis and Stroke |Haemorrhagic Stroke |Stroke Thrombolysis |Hyperacute Stroke Care
🧠 Introduction
- 💡 Stroke medicine evolved rapidly with the introduction of CT scanning, enabling clinicians to distinguish between ischaemic and haemorrhagic strokes quickly and safely. Non-contrast CT (NCCT) is the initial investigation of choice for nearly all suspected strokes.
- ⚙️ CT imaging is central to acute stroke management - it determines stroke type, rules out mimics, and guides emergency therapies such as thrombolysis or thrombectomy.
- 📜 Before CT, differentiating stroke subtypes relied on clinical signs or even post-mortem findings. Early diagnostic methods (e.g. pineal calcification displacement) were crude and unreliable.
📚 History of CT Imaging
- 🧑🔬 Sir Godfrey Hounsfield developed the first CT scanner in 1972 - funded by EMI’s Beatles record profits 🎸.
- 🧩 The first clinical CT scan in 1971 (Atkinson Morley Hospital, London) diagnosed a cerebral cyst - a landmark moment in neuroradiology.
- 🏥 By the late 1980s, CT became routine in major hospitals, revolutionising stroke diagnosis and management.
⚙️ Technical Aspects of CT
- 🌀 A CT scanner uses a rotating X-ray tube and detectors to capture cross-sectional images of the body, reconstructed by a computer into slices.
- 🔁 Helical (spiral) CT introduced in the 1990s enabled continuous scanning for 3D reconstructions - essential for vascular imaging.
- 📏 Image density is expressed in Hounsfield Units (HU):
- Air = -1000 HU
- Water = 0 HU
- Grey matter ≈ +35 HU
- Acute haemorrhage ≈ +70 HU
- Bone = +400 to +3000 HU
☢️ Radiation Exposure
- CT involves ionising radiation and is regulated under IRMER in the UK - only to be performed when clinically justified.
- 🧮 A typical CT head ≈ 2 mSv → roughly equivalent to 100 chest X-rays.
- 🌍 Natural background radiation ≈ 3.1 mSv/year for comparison.
| Scan Type | Approx. Radiation Dose (mSv) |
|---|---|
| 🌍 Natural Background | 3.1 / year |
| 🧠 Brain CT | 2.0 |
| 🫁 Chest CT | 7.0 |
| 🫀 Chest + Abdomen + Pelvis | 21.0 |
🏥 CT in Acute Stroke
- CT is first-line for suspected stroke - rules out haemorrhage before thrombolysis or thrombectomy.
- Indications: sudden focal neurological deficit, decreased consciousness, headache, or anticoagulant use.
- ⚠️ Early CT may appear normal within first 6 hours of ischaemia - correlate with clinical findings.
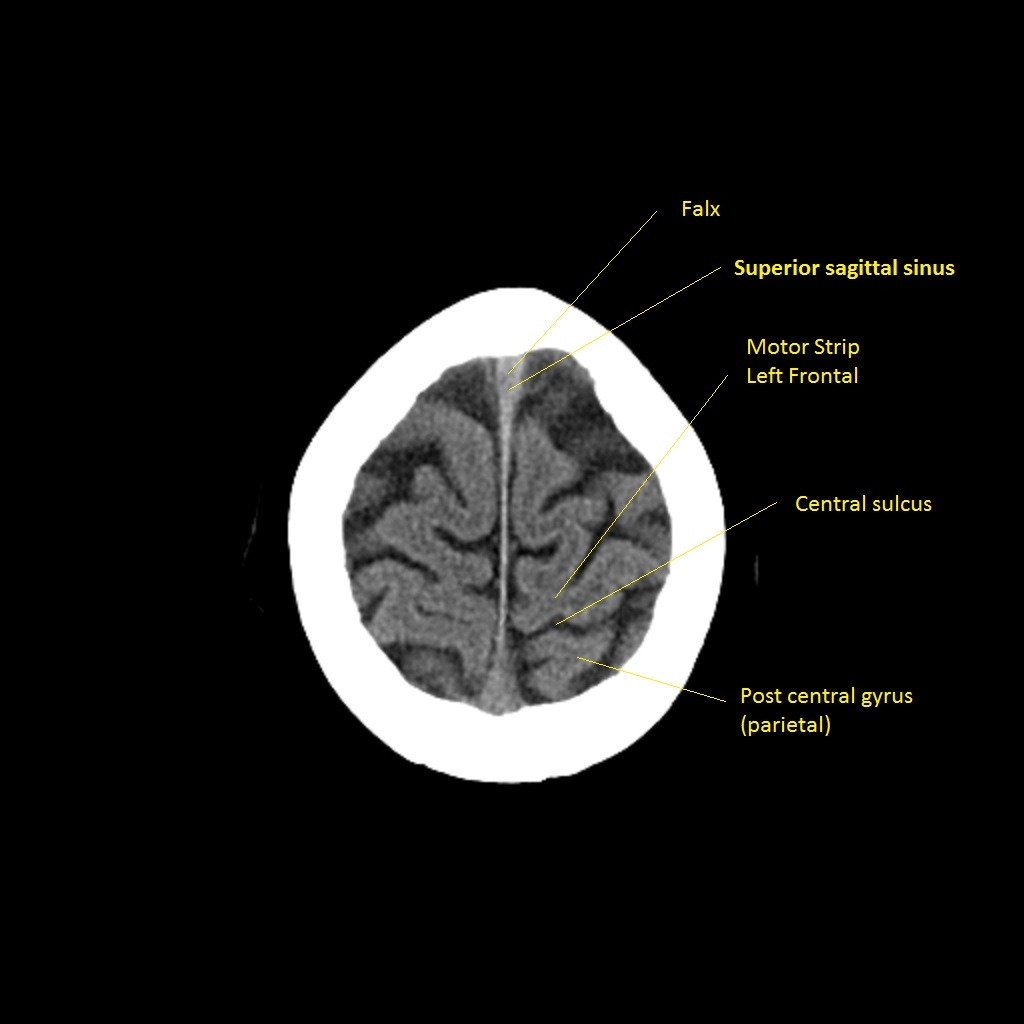
🔍 CT Interpretation Tips
🧩 Review CT systematically from vertex to base. Look for hyperdensities (clots), hypodensities (oedema or infarction), and mass effect. Always exclude mimics such as subdural haematoma or tumour before giving thrombolysis.
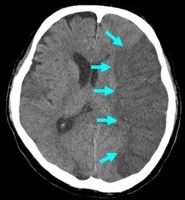
🧠 Early Signs of Ischaemia on CT
- ⚡ Hyperdense MCA sign: Thrombus in middle cerebral artery - earliest visible clue.
- 🌫️ Loss of grey-white differentiation: Early cytotoxic oedema, especially in cortex or basal ganglia.
- 🌀 Insular ribbon sign: Blurring between insular cortex and adjacent white matter.
- 🌊 Effacement of sulci: Local swelling and oedema flattening cortical grooves.
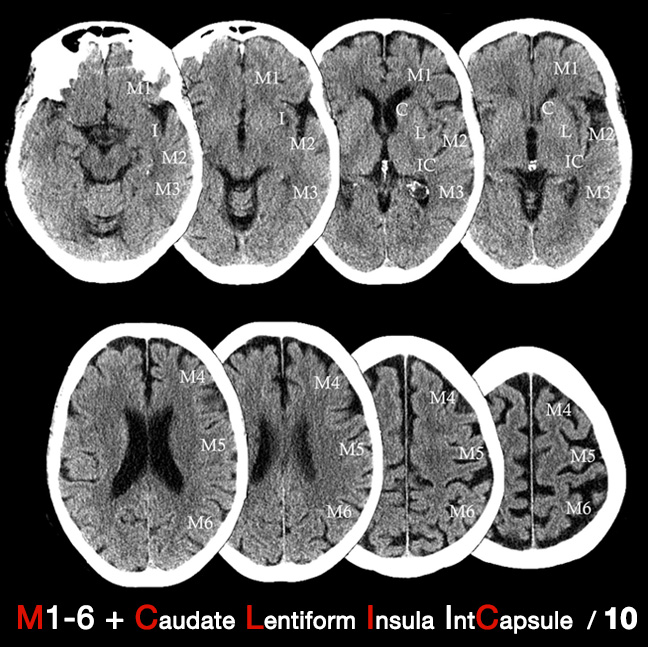
🧮 ASPECTS Score
The Alberta Stroke Program Early CT Score (ASPECTS) assesses early ischaemic change in MCA territory. • Score = 10 (normal), decreasing with extent of infarction. • ASPECTS ≤ 7 → poorer prognosis & higher risk of post-thrombolysis haemorrhage.
🩸 CTA & CT Perfusion (CTP)
- 🧩 CT Angiography (CTA): Maps arteries from aortic arch → Circle of Willis; identifies clots, dissections, or stenosis. Essential before thrombectomy.
- 🎯 CT Perfusion (CTP): Measures blood flow (CBF), volume (CBV), and mean transit time (MTT). Differentiates core infarct vs. penumbra (salvageable tissue).
⚠️ Limitations of CT
- ❌ May miss small brainstem strokes or subtle early cortical ischaemia.
- 🧩 False negatives possible in first few hours; false positives from leukoaraiosis in elderly.
🕓 Later CT Signs (6–24 hours)
- ⬜ Hypodense areas become obvious due to cytotoxic and vasogenic oedema.
- 💔 Haemorrhagic transformation may occur, especially in large infarcts or with anticoagulant use.

💡 Teaching tip: - NCCT remains the first-line scan for stroke - fast, reliable, and accessible. - Subtle early changes demand a trained eye and careful side-by-side comparison. - Combine imaging findings with clinical localisation for accurate decision-making.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery