Related Subjects:
|Drug Toxicity - clinical assessment
|Metabolic acidosis
|Aspirin or Salicylates toxicity
|Ethylene glycol toxicity
|Ethanol toxicity
|Methanol toxicity
|Ricin toxicity
|Carbon Tetrachloride Toxicity
|Renal Tubular Acidosis
|Lactic acidosis
|Iron Toxicity
|Tricyclic Antidepressant Toxicity
|Opiate Toxicity
|Carbon monoxide Toxicity
|Benzodiazepine Toxicity
|Paracetamol (Acetaminophen) toxicity
|Amphetamine toxicity
|Beta Blocker toxicity
|Calcium channel blockers toxicity
|Cannabis toxicity
|Cyanide toxicity
|Digoxin Toxicity
|Lithium Toxicity
|NSAIDS Toxicity
|Ecstasy toxicity
|Paraquat toxicity
|Quinine toxicity
|SSRI Toxicity
|Theophylline Toxicity
|Organophosphate (OP) Toxicity
|Toxin elimination by dialysis
|Drug Toxicity with Specific Antidotes
🧪 Lead (Pb) toxicity - Prevention is paramount: even very low exposures can impair neurodevelopment, and chelation cannot undo established brain injury. 🧠🚫
🔎 About
- Lead is widespread: paint, pipes, batteries, solder, ammunition, pottery glazes, cosmetics, remedies, soil, firing ranges.
- Historic curios: “sugar of lead” (acetate) sweetened wine; “mad hatter” syndrome was likely heavy-metal neurotoxicity.
- Distribution: >95% stored in bone/teeth (long half-life); mobilises in pregnancy, lactation, illness, osteoporosis. 🦴
🧒 Common Exposure Sources
- Children: Old paint/dust, contaminated soil, lead pipes, imported spices/cosmetics, pottery, folk remedies.
- Adults: Battery smelting, radiator/e-waste repair, construction/renovation, stained glass, shooting ranges, ammo reloading.
- Unusual: Retained bullets (esp. intra-articular), lead-soldered moonshine stills.
🩺 Clinical Features – Systems
| System | Features |
|---|
| 🧠 Neuro | Irritability, headache, memory loss, encephalopathy (↑ICP, seizures), peripheral neuropathy → wrist/foot drop |
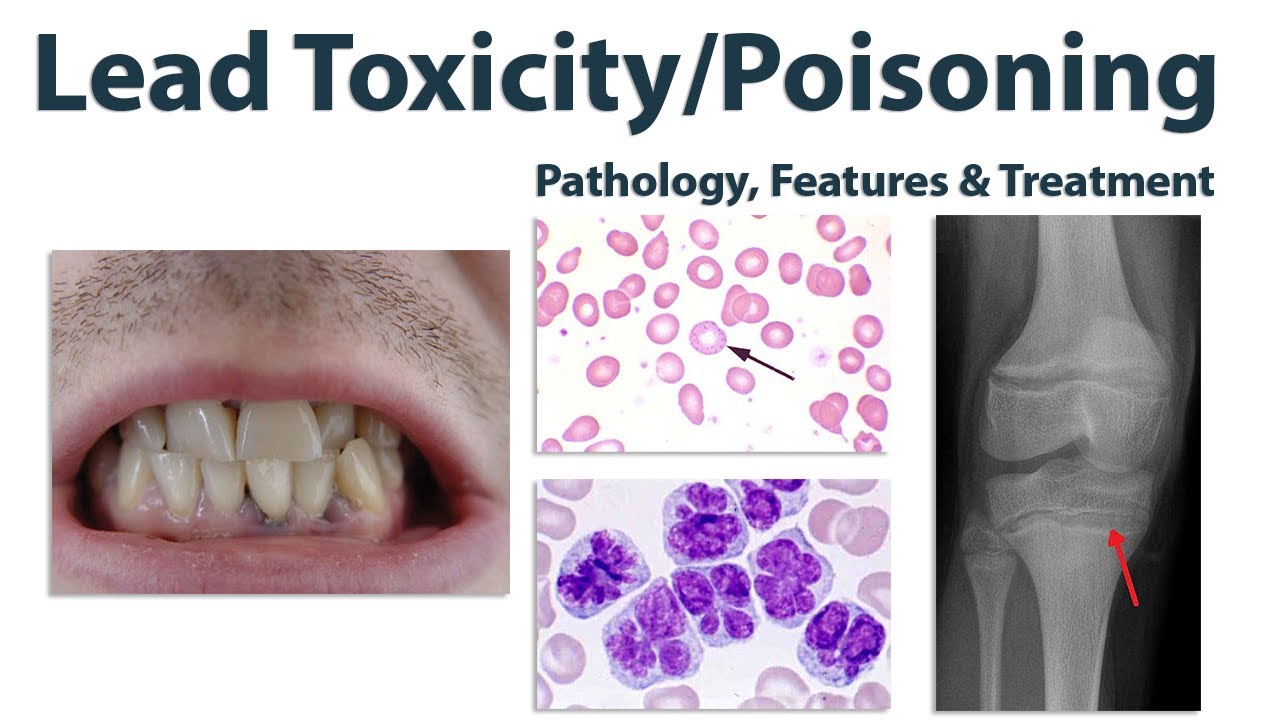
| 🩸 Haematology | Microcytic hypochromic anaemia, haemolysis, basophilic stippling |
| 🦷 Oral | Burton line (blue-black gingival margin) |
| 🍽️ GI | Colicky abdominal pain, constipation > diarrhoea, anorexia, vomiting |
| 🧂 Renal | Tubular dysfunction, proteinuria, hyperuricaemia → “saturnine gout” |
| 🦴 Skeletal (children) | Dense metaphyseal “lead lines” on X-rays |
| ❤️ Cardio-metabolic | Hypertension, dyslipidaemia risk |
| 🤰 Reproductive | Infertility, miscarriage, prematurity, LBW; placental & breast milk transfer |
🧪 Investigations
- Blood Lead Level (BLL): Diagnostic test (venous). Units: µg/dL. 10 µg/dL ≈ 0.48 µmol/L.
- Children: CDC threshold ≥3.5 µg/dL (UK often ≥5 µg/dL) → trigger interventions.
- Ancillary: FBC (microcytosis, basophilic stippling), iron studies, renal profile, uric acid.
- ↑ Free/Zinc protoporphyrin, ↑ ALA/copro-porphyrins (higher exposures).
- Imaging: Abdo X-ray if pica ingestion (radio-opaque flecks); long-bone films in children.
⚠️ When to Worry
- Children:
- ≥3.5 µg/dL: trigger environmental/nutritional intervention
- 45–69 µg/dL: usually oral succimer (DMSA)
- ≥70 µg/dL or encephalopathy: hospitalise, IV CaNa2EDTA ± dimercaprol (BAL)
- Adults: Remove from exposure at elevated levels; consider chelation if symptomatic or ≥80–100 µg/dL.
💊 Chelation Agents (comparison)
| Agent | Route | Indication | Cautions |
|---|
| Succimer (DMSA) | PO | Moderate elevations, children/adults | LFTs, neutropenia risk, “rebound” common |
| CaNa2EDTA | IV | Severe toxicity, encephalopathy (with BAL) | Renal monitoring, must use calcium salt |
| Dimercaprol (BAL) | IM | Severe encephalopathy (with EDTA) | Peanut oil carrier, painful, avoid in G6PD |
| DMPS / D-Penicillamine | PO/IV | Used in some regions | Not first-line everywhere |
🛠️ Management Summary
- 🛑 Immediate: Remove exposure (home remediation, PPE, safe work practices).
- 🥦 Nutritional: Correct iron deficiency, ensure calcium/vitamin C intake.
- 💊 Chelation: Succimer, EDTA, BAL (see table).
- 🚰 GI decontamination: Whole-bowel irrigation if ingestion suspected.
- 📈 Follow-up: Serial BLLs, neurodevelopment checks in children, occupational health monitoring in adults.
🚨 Complications
- Children: irreversible cognitive delay, behavioural problems, hearing loss.
- Adults: neuropathy, CKD, hypertension, gout.
- Pregnancy: prematurity, miscarriage, foetal growth restriction.
🏛️ Prevention & Public Health
- Primary prevention: lead-safe housing renovation, water pipe replacement, dust control, PPE for high-risk occupations.
- Reportable condition → public health investigation of home/workplace.
💡 Pearls & Pitfalls
- Even “low” BLLs are harmful - act environmentally even if chelation not indicated.
- Iron deficiency ↑ Pb absorption - always check ferritin.
- Pregnancy: mobilised bone lead; involve toxicology & obstetrics.
- Neurologic injury may persist despite chelation - set expectations, ensure support. 🎯
Cases - Lead Toxicity
- Case 1: A 6-year-old boy is brought with abdominal pain, constipation, and irritability. Examination: pale, blood film shows basophilic stippling. Family lives in an old house with peeling paint. Blood lead level: 70 µg/dL.
Management: Hospital admission, oral succimer (DMSA) for chelation, iron supplementation, and referral to environmental health.
Outcome: Symptoms resolve within 2 weeks, lead levels fall. Safe rehousing arranged until home repairs completed.
- Case 2: A 45-year-old battery recycling worker presents with fatigue, wrist drop, and Burton’s line on gums. Blood lead level: 95 µg/dL.
Management: Removed from exposure, IV EDTA chelation commenced, and occupational health involved. Physiotherapy for neuropathy.
Outcome: Lead levels fall; partial improvement in neuropathy, but some persistent weakness. Redeployed to non-exposure duties.
- Case 3: A 3-year-old child presents with seizures, developmental regression, and vomiting. Parents report she frequently chews old painted window sills. Blood lead level: 120 µg/dL. CT head is normal, but LP excluded infection. Management: PICU admission, seizure control with IV benzodiazepines, IV EDTA plus dimercaprol (British anti-Lewisite) for chelation, aggressive hydration, and correction of metabolic acidosis. Social services and public health urgently notified. Outcome: Seizures controlled, lead levels decline after therapy, but neurocognitive assessment reveals persistent learning difficulties. Long-term paediatric neurology follow-up arranged.
Teaching Commentary 🧑⚕️
Lead poisoning severity ranges from mild GI upset and anaemia (Case 1), to neuropathy in chronic occupational exposure (Case 2), to life-threatening encephalopathy in children (Case 3). Lead interferes with haem synthesis and is directly neurotoxic, especially to the developing brain. Management always combines eliminating exposure, chelation therapy (DMSA, EDTA, BAL), and public health interventions. Outcomes vary - neurological sequelae are common after severe childhood exposure, underlining the importance of early detection and prevention.
