Related Subjects:
|Cardiology Examination
|Cardiology History Taking
|Epstein-Barr Virus infection
|Cytomegalovirus (CMV) infections
Examination of the spleen helps detect splenomegaly, assess consistency, and guide investigations. Key OSCE pearl: always start palpation in the right iliac fossa as the spleen enlarges diagonally towards it.
🛠️ Preparation
- Ensure privacy & obtain consent.
- Explain the procedure clearly to the patient.
- Position: supine, arms by side, abdomen exposed, comfortable.
👀 Inspection
- Look for visible swelling/mass in the LUQ.
- Ask patient to take a deep breath - observe LUQ contour changes.
✋ Palpation
- Stand on patient’s right side.
- Start in RIF, move diagonally towards left costal margin.
- Ask patient to take deep breaths - feel spleen tip descending.
- If not felt → roll patient into right lateral decubitus, support back, palpate again.
🥁 Percussion
- Percuss Traube’s space (6th rib → left costal margin, anterior axillary line).
- Normal: resonant. Dullness suggests splenomegaly.
📋 Common Findings
- Normal: Non-palpable spleen, resonant percussion.
- Splenomegaly: Palpable below costal margin, enlarges towards RIF, notched edge may be felt.
- Consistency:
- Soft/tender → acute infection/congestion.
- Firm → chronic leukaemia, myeloproliferative disease.
- Massive (>8 cm below costal margin) → CML, Myelofibrosis, Malaria.
📝 Documentation
- Presence/absence of splenomegaly.
- Size (how many cm below costal margin).
- Consistency, tenderness, edge.
- Any associated findings (hepatomegaly, lymphadenopathy, ascites).
🧾 Causes of Splenomegaly
Mnemonic (Massive Splenomegaly): "MMM" = Myelofibrosis, Malaria, Myeloid leukaemia (CML).
- Massive: Myelofibrosis, Chronic Myeloid Leukaemia, Malaria, Visceral leishmaniasis (Kala-azar).
- Moderate: Portal hypertension, Thalassaemia, Haematological malignancy (Lymphoma, CLL, Polycythaemia vera).
- Mild: Viral infections (EBV, CMV), bacterial endocarditis, autoimmune (SLE, RA), storage disorders (Gaucher’s, Niemann-Pick).
📊 Investigations
| Investigation | Finding |
|---|
| FBC | Pancytopenia (hypersplenism), anaemia |
| Blood film | Abnormal cells (e.g., blasts in leukaemia, parasites in malaria) |
| LFTs | Signs of cirrhosis/portal hypertension |
| Ultrasound/CT | Confirm splenomegaly, assess structure |
| Bone marrow biopsy | Myeloproliferative / infiltrative causes |
| Serology | Infections: EBV, malaria, kala-azar |
⚕️ Management
- Treat underlying cause (e.g., malaria → antimalarials, CML → tyrosine kinase inhibitors).
- Splenectomy for trauma, refractory haematological disease (ITP, spherocytosis).
- Always ensure post-splenectomy vaccines & prophylaxis if spleen removed.
📈 Summary
Spleen exam = Inspect 👀 → Palpate ✋ (RIF→LUQ, with inspiration) → Percuss 🥁 (Traube’s space).
Normal spleen not palpable.
Massive splenomegaly → think MMM (Myelofibrosis, Malaria, Myeloid leukaemia).
Always document fully & link findings to systemic disease.
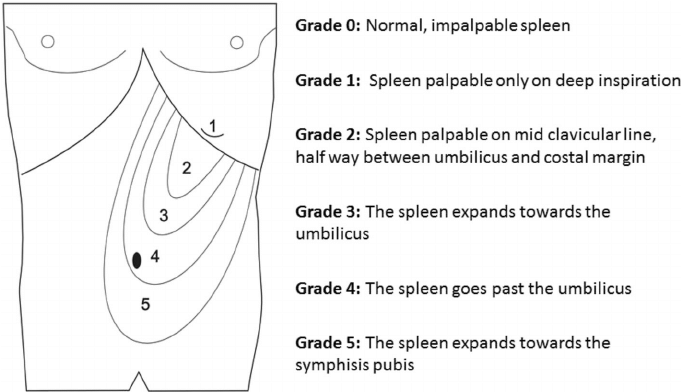
🖼️ Diagram