
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute Appendicitis ✅
Related Subjects:Acute Cholecystitis |Acute Appendicitis |Acute Appendicitis in Children |Chronic Peritonitis |Acute Abdominal Pain |Chronic Peritonitis |Abdominal Aortic Aneurysm |Ectopic Pregnancy |Acute Cholangitis |Acute Abdominal Pain |Penetrating Abdominal Trauma |Acute Pancreatitis |Acute Diverticulitis
Overview / Definition
Acute appendicitis is inflammation of the vermiform appendix, usually triggered by luminal obstruction and bacterial overgrowth. It is a common cause of acute abdominal pain requiring emergency surgical assessment. Untreated, it can progress to gangrene, perforation, peritonitis, sepsis, and abscess. Because symptoms overlap with gastroenteritis, urinary, and gynaecological disease, diagnosis relies on a combination of clinical assessment + symptom trajectory supported by targeted investigations.
Epidemiology
- 📊 Lifetime risk: ~7–8%; higher in men (~8.6%) than women (~6.7%).
- 👥 Age: Peak in teens/early adulthood; extremes of age have higher perforation rates and atypical presentations.
- 🔍 Diagnostic reality: Negative appendicectomy historically 10–20%, now reduced with modern imaging.
Anatomy of the Appendix
- 📍 Blind-ended tube from caecum near the ileocaecal valve; variable length (~6–10 cm).
- 🧭 Positions: retrocaecal (most common), pelvic, pre-/post-ileal, paracaecal – affects symptom localisation.
- 🩸 Blood supply: appendicular artery (end-artery branch of ileocolic) → rapid ischaemia if obstruction rises.
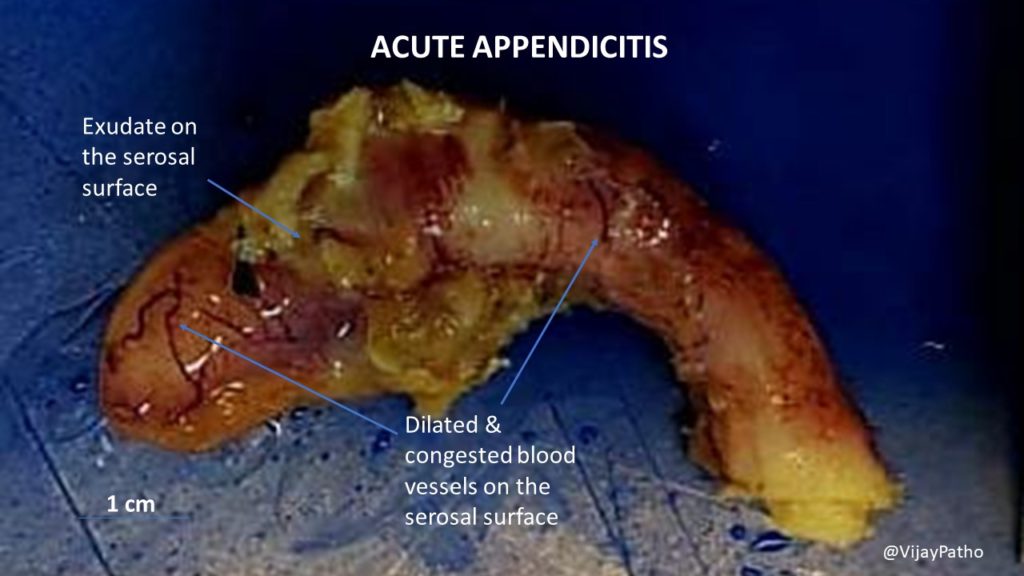
Pathophysiology
Sequence: obstruction → mucus accumulation → ↑ intraluminal pressure → venous congestion → bacterial proliferation → mural ischaemia → gangrene → perforation. Visceral pain starts peri-umbilically; once parietal peritoneum is involved, pain localises to RIF. Key teaching: appendicitis is dynamic; a single exam can be misleading, so re-examination and escalation are essential.
Aetiology / Causes
- 🚧 Luminal obstruction: faecolith, lymphoid hyperplasia (children), rarely tumour.
- 🦠 Infective triggers: viral illness → lymphoid hyperplasia; gut flora contribute after obstruction.
- 🐛 Parasites: Enterobius occasionally implicated.
Risk Factors
- 👶 Children & 👵 older adults: higher risk of delayed diagnosis/perforation.
- 💊 Immunosuppression/steroids: blunted inflammatory response (normal WCC/fever misleading).
- 🤰 Pregnancy: atypical localisation; broader differential.
🩺 Clinical Features
- ➡️ Pain: peri-umbilical → RIF; worsens with movement/cough.
- 🤢 GI: anorexia, nausea; vomiting follows pain (vs gastroenteritis).
- 🌡️ Systemic: low-grade fever, tachycardia; severe sepsis suggests perforation/abscess.
- 💩 Bowel/urinary: diarrhoea/tenesmus (pelvic appendix), dysuria (bladder/ureter irritation).
Typical vs Atypical Presentations
- ✅ Typical: migration, RIF tenderness, anorexia, rising inflammatory markers.
- ⚠️ Atypical: retrocaecal (flank/back pain), pelvic (suprapubic pain, diarrhoea, urinary), elderly (subtle), pregnancy (pain shifts cephalad), immunosuppressed (few signs).
Pain Migration & Neuroanatomy
Early visceral pain via sympathetic afferents → peri-umbilical (T10). Parietal peritoneum involvement → sharper localised RIF pain. This links exam findings with disease stage and complication risk.
Examination Findings
- 👆 RIF tenderness (McBurney’s), percussion/cough tenderness, guarding, rebound.
- ↪️ Rovsing’s sign: LLQ palpation → RIF pain.
- 🦵 Psoas sign (retrocaecal), obturator sign (pelvic).
- 🩺 Male: testicular exam; Female: gynae assessment as appropriate.
Special Populations
- 👶 Children: mimic gastroenteritis; perforate earlier; use paediatric scores, USS-first.
- 👵 Elderly: subtle pain/fever; early imaging advised.
- 🤰 Pregnancy: pain may shift; USS first, MRI if equivocal; do not ignore strong clinical suspicion.
- 💊 Immunocompromised: low threshold for imaging/senior review.
Differential Diagnosis
- 🦠 Gastroenteritis, mesenteric adenitis, constipation.
- 🧻 UTI/pyelonephritis, ureteric stone.
- 🩸 Gynae: ectopic, ovarian torsion/cyst, PID.
- 🧠 IBD (terminal ileitis), Meckel’s diverticulitis, right-sided diverticulitis.
- 🔁 Older adults: consider caecal/appendiceal tumour.
🔎 Investigations
Blood Tests
- 🩸 FBC, CRP, U&E, LFTs, amylase/lipase (broader acute abdomen screen).
- 🧪 Lactate/VBG if sepsis or concern for ischaemia/perforation.
- 🧾 Group & save / crossmatch if operative likelihood.
Urinalysis
- 💧 Identify UTI; mild haematuria possible from ureteric irritation.
Pregnancy Testing
- 🤰 β-hCG for all females of reproductive potential – ectopic pregnancy until excluded.
Imaging
- 🖥️ CT A/P (adults): high accuracy, identifies complications and alternative diagnoses.
- 🩻 Ultrasound: first-line in children/pregnancy; operator dependent.
- 🧲 MRI (pregnancy): when USS inconclusive and clinical suspicion persists.
Risk Stratification / Clinical Scoring
- 📐 Alvarado, AIR, paediatric scores guide observation vs imaging vs urgent surgery.
- ⚠️ Scores are adjuncts – do not override clear peritonism or deterioration.
Initial Management
| ⚡ Initial Management |
|---|
|
Antibiotic Therapy
- 💊 Follow local guidance; start promptly if complicated appendicitis suspected.
- ✅ Simple/uncomplicated: peri-op prophylaxis; no post-op antibiotics often needed.
- 💥 Complex/perforated/abscess/sepsis: IV broad-spectrum, step-down guided by clinical response (~3–7 days).
Surgical Management
- 🔪 Laparoscopic appendicectomy: standard, faster recovery, fewer wound infections.
- 🟠 Open appendicectomy: selected cases (dense adhesions, complex disease).
- 🕒 Timing: urgent intervention for unstable/septic/peritonitic; elective/urgent window for stable uncomplicated cases.
Non-operative (Antibiotics-First) Management
- 🟡 Selected, uncomplicated, imaging-confirmed cases with shared decision-making and follow-up.
- 🔁 Counsel on recurrence risk; appendicolith increases failure risk.
- 🚫 Not for peritonism, sepsis, perforation, abscess, or diagnostic uncertainty.
Appendix Mass / Abscess
- 🧱 Tender RIF mass, persistent fever, raised CRP; CT shows phlegmon ± collection.
- 🛡️ IV antibiotics, bowel rest; IR drainage if drainable.
- 🔎 Colonic assessment in older adults to exclude malignancy.
⚠️ Complications
- 💥 Perforation → peritonitis, septic shock.
- 🛡️ Abscess/phlegmon, wound infection, intra-abdominal collections.
- 🧵 Adhesions → late SBO (rare).
- 🩸 VTE risk from inflammation/immobility.
Post-operative Care
- 🚶 Early mobilisation, analgesia, antiemetics, diet as tolerated.
- 🩺 Monitor fever, pain, ileus, wound; low threshold for imaging if deteriorating.
- 🧪 Review histology (rare neoplasm alters follow-up).
- 🏠 Discharge: clear safety net for worsening symptoms.
Outcomes / Prognosis
- ✅ Prompt uncomplicated appendicitis → excellent outcomes, short admission.
- ⏱️ Delayed diagnosis → higher perforation, abscess, prolonged antibiotics, longer stay.
- 👶👵 Children/older adults → higher complication rates from diagnostic delay/atypical features.
Common Pitfalls / Missed Diagnoses
- ⚠️ Normal early CRP/WCC, especially <12 h or immunosuppressed.
- ⚠️ Mistaking appendicitis for gastroenteritis; ignore focal/progressive pain/peritonism.
- ⚠️ Women: exclude ectopic pregnancy/ovarian pathology.
- ⚠️ Older adults: consider tumour-associated appendicitis.
Case-Based Examples
Case 1 (classic): 21-year-old, peri-umbilical → RIF pain, anorexia, low-grade fever, guarding; WCC/CRP raised; CT confirms uncomplicated appendicitis → fluids, analgesia, peri-op antibiotics, laparoscopic appendicectomy.
Case 2 (pregnancy): 22 weeks, RUQ/right flank pain, vomiting; USS equivocal; MRI confirms appendicitis → early surgical management with obstetric awareness.
Case 3 (mass/abscess): 55-year-old, 5 days symptoms, RIF mass; CT: phlegmon + small collection → IV antibiotics ± drainage; follow-up colonic evaluation, selective interval surgery.
Key Learning Points / Exam Pearls
- 🧠 Appendicitis is trajectory-based: repeat exams and escalation with deterioration are critical.
- 🧭 Appendix position explains atypical symptoms (retrocaecal = flank/back; pelvic = urinary/diarrhoea).
- 🤰 Pregnancy: USS first, MRI if equivocal; do not ignore strong clinical suspicion.
- 🩺 Early analgesia is safe and does not invalidate the exam.
- 🟡 Antibiotics-first = selected uncomplicated cases; perforation/sepsis/peritonism = surgical pathway.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery