
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Vascular System
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The vascular system is a closed network of arteries, arterioles, capillaries, venules, and veins that delivers oxygen and nutrients, removes metabolic waste, transports hormones, and maintains blood pressure and tissue perfusion. Its performance depends on vessel wall structure (especially smooth muscle and elastin), endothelial signalling, and coordinated neural–hormonal control of vascular tone and blood volume.
🏗️ 1) Vascular Anatomy: The “Tree” from Heart to Tissue and Back
- Arteries → carry blood away from the heart under high pressure.
- Arterioles → the main resistance vessels; regulate flow into each organ.
- Capillaries → the main exchange vessels; nutrients/gases/waste cross here.
- Venules → collect blood from capillary beds; important in inflammation.
- Veins → low-pressure capacitance vessels that return blood to the heart.
💡 Clinical frame: arteries determine pressure, arterioles determine distribution, capillaries determine exchange, and veins determine volume reserve.
🧱 2) Vessel Wall Structure (Shared Blueprint)
- Tunica intima:
- Endothelium + basement membrane.
- Key role in thrombosis control, inflammation, and vasomotor tone.
- Tunica media:
- Vascular smooth muscle + elastin/collagen.
- Controls vasoconstriction/vasodilation (thus resistance and BP).
- Tunica adventitia:
- Connective tissue; contains vasa vasorum (for large vessels) and nerves.
🟥 3) Arteries: Types and Functional Specialisation
🟧 Elastic (Conducting) Arteries
- Examples: aorta, pulmonary artery, common carotids.
- High elastin content → “Windkessel” effect:
- Stretch in systole stores energy.
- Recoil in diastole maintains forward flow and diastolic pressure.
🟨 Muscular (Distributing) Arteries
- Examples: femoral, radial, coronary arteries.
- More smooth muscle → regulate regional distribution of blood flow.
🟥 Arterioles (Resistance Vessels)
- Small lumen + thick smooth muscle.
- Primary determinant of systemic vascular resistance (SVR) and therefore arterial BP.
- Highly responsive to:
- Sympathetic tone (α1 constriction)
- Local metabolites (adenosine, CO₂, H⁺, K⁺, lactate)
- Endothelial factors (NO, endothelin)
🟦 4) Capillaries and Microcirculation (Where Exchange Happens)
Capillaries are single-layer endothelial tubes designed for diffusion and bulk flow. Exchange occurs across the endothelial barrier and its glycocalyx, driven by concentration gradients and pressure gradients.
🔬 Capillary Types
- Continuous (tight junctions, low permeability): skeletal muscle, skin, lung, CNS (BBB is specialised).
- Fenestrated (pores increase permeability): kidney, endocrine glands, small intestine.
- Sinusoidal/Discontinuous (very permeable): liver, spleen, bone marrow.
🚪 Precapillary Sphincters and Flow Distribution
- Local smooth muscle at capillary entrances.
- Direct flow to areas with high metabolic demand (e.g., working muscle).
💧 Starling Forces (Fluid Movement)
Fluid movement across capillaries reflects a balance between hydrostatic pressure pushing fluid out and oncotic pressure pulling fluid in. When outward forces exceed inward forces, net filtration occurs → interstitial fluid; lymphatics return excess fluid to circulation.
- Increased capillary hydrostatic pressure (e.g., heart failure, venous obstruction) → oedema.
- Reduced plasma oncotic pressure (e.g., low albumin from liver disease, nephrotic syndrome) → oedema.
- Increased capillary permeability (e.g., inflammation, sepsis) → protein-rich oedema.
- Lymphatic obstruction (e.g., malignancy, filariasis) → lymphoedema.
🟪 5) Venous System (Capacitance and Return)
- Veins contain most of the blood volume at rest (capacitance reservoir).
- Thin walls, larger lumen, lower smooth muscle than arteries.
- Valves (especially in legs) prevent backflow.
⬆️ Venous Return: How Blood Gets Back to the Heart
- Skeletal muscle pump + valves (walking compresses deep veins).
- Respiratory pump: inspiration lowers intrathoracic pressure → draws venous blood to thorax.
- Sympathetic venoconstriction increases stressed volume → boosts venous return and preload.
📌 Clinical link: venodilation (e.g., nitrates) reduces venous return (preload) → helpful in angina and pulmonary oedema.
🧠 6) Control of Vascular Tone (Who Sets the Diameter?)
🧬 Endothelium (A “Hidden Endocrine Organ”)
- Nitric oxide (NO) → vasodilation (↑ cGMP), inhibits platelet aggregation.
- Prostacyclin (PGI₂) → vasodilation + anti-platelet effect.
- Endothelin-1 → potent vasoconstrictor.
- ACE/Angiotensin signalling interacts with endothelial tone and remodelling.
🧠 Neural Control
- Sympathetic:
- α1 receptors → vasoconstriction (skin, gut, kidney).
- β2 receptors → vasodilation (skeletal muscle, mainly via adrenaline).
- Parasympathetic: minimal direct effect on most systemic vessels (exceptions in specific beds).
🧪 Hormonal Control
- RAAS: angiotensin II constricts; aldosterone retains salt/water.
- ADH (vasopressin): vasoconstriction at higher concentrations + water retention.
- ANP/BNP: vasodilation + natriuresis.
❤️ 7) Haemodynamics: The Core Relationships
Key equations explain many bedside phenomena:
- Blood pressure: MAP ≈ CO × SVR
- Flow: Q = ΔP / R
- Resistance: (Poiseuille) R ∝ 1 / r⁴ → tiny radius change massively alters resistance.
- Shear stress stimulates NO release → adaptive vasodilation.
🩺 Pulse Pressure and Arterial Stiffness
- Pulse pressure rises with arterial stiffness (e.g., ageing, atherosclerosis).
- Loss of elastic recoil → higher systolic and lower diastolic pressures.
🧫 8) Lymphatics (Often Forgotten, Always Important)
- Return excess interstitial fluid and proteins to circulation.
- Central for immune surveillance (lymph nodes).
- Failure → lymphoedema (classically non-pitting later on, skin thickening).
⚠️ 9) Clinical Correlations (High-Yield)
- Atherosclerosis: endothelial dysfunction + lipid deposition → plaque; can reduce flow or rupture → thrombosis.
- Shock states:
- Hypovolaemic: low preload → low CO.
- Cardiogenic: pump failure → low CO, high filling pressures.
- Distributive (sepsis): low SVR from vasodilation + leak.
- Hypertension: chronic arteriolar constriction/remodelling increases SVR; damages end organs via shear and microvascular injury.
- Venous disease: valve failure → venous hypertension → oedema, varicosities, ulcers (gaiter area).
- DVT/PE: venous stasis + endothelial injury + hypercoagulability (Virchow’s triad).
📊 Quick Revision Table
| Vessel Type | Key Structure | Main Function | Clinical Link |
|---|---|---|---|
| Elastic arteries | High elastin | Buffer pulsatile flow (Windkessel) | Stiffness → wide pulse pressure |
| Muscular arteries | More smooth muscle | Distribute flow to organs | Vasospasm, atherosclerosis |
| Arterioles | Small radius, thick media | Set SVR and regional perfusion | HTN, shock physiology |
| Capillaries | Single endothelial layer | Exchange + filtration | Oedema (Starling imbalance) |
| Veins | Large lumen, valves | Volume reservoir + return | DVT, varicose veins |
| Lymphatics | Valved channels + nodes | Return fluid/protein, immunity | Lymphoedema |
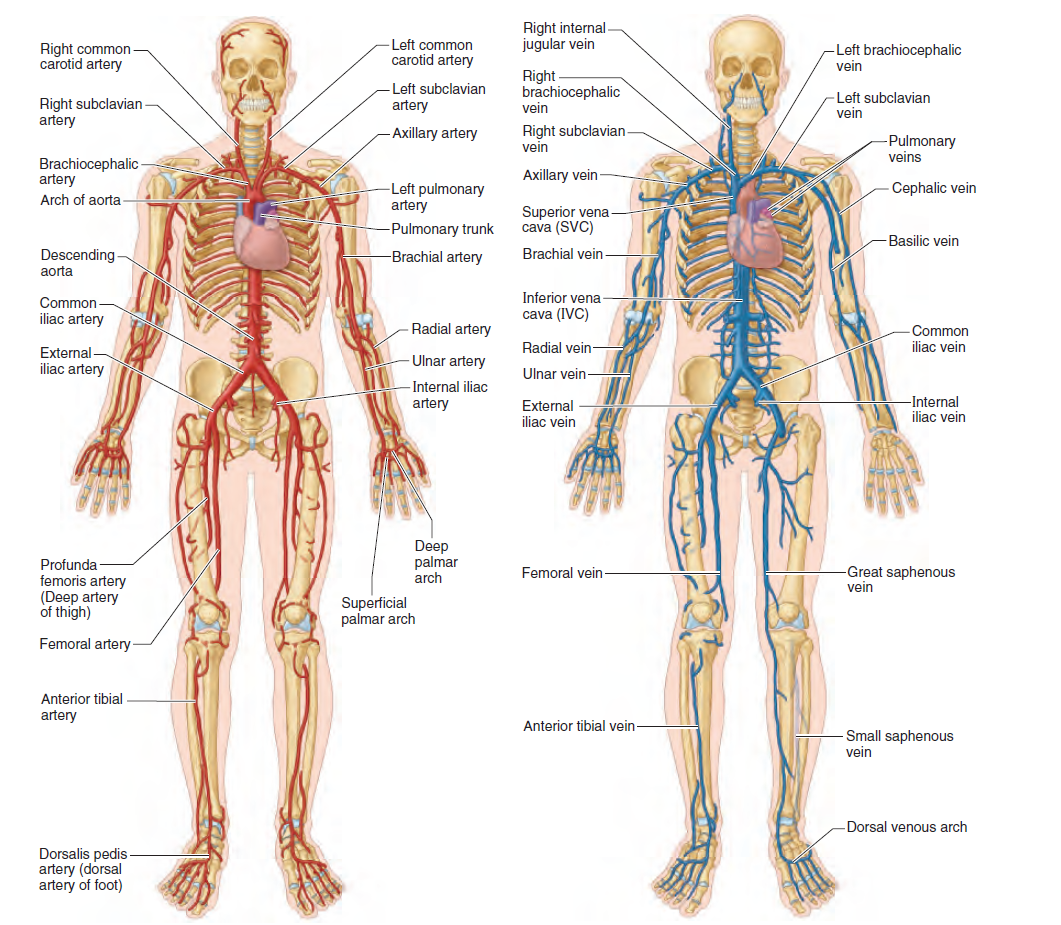
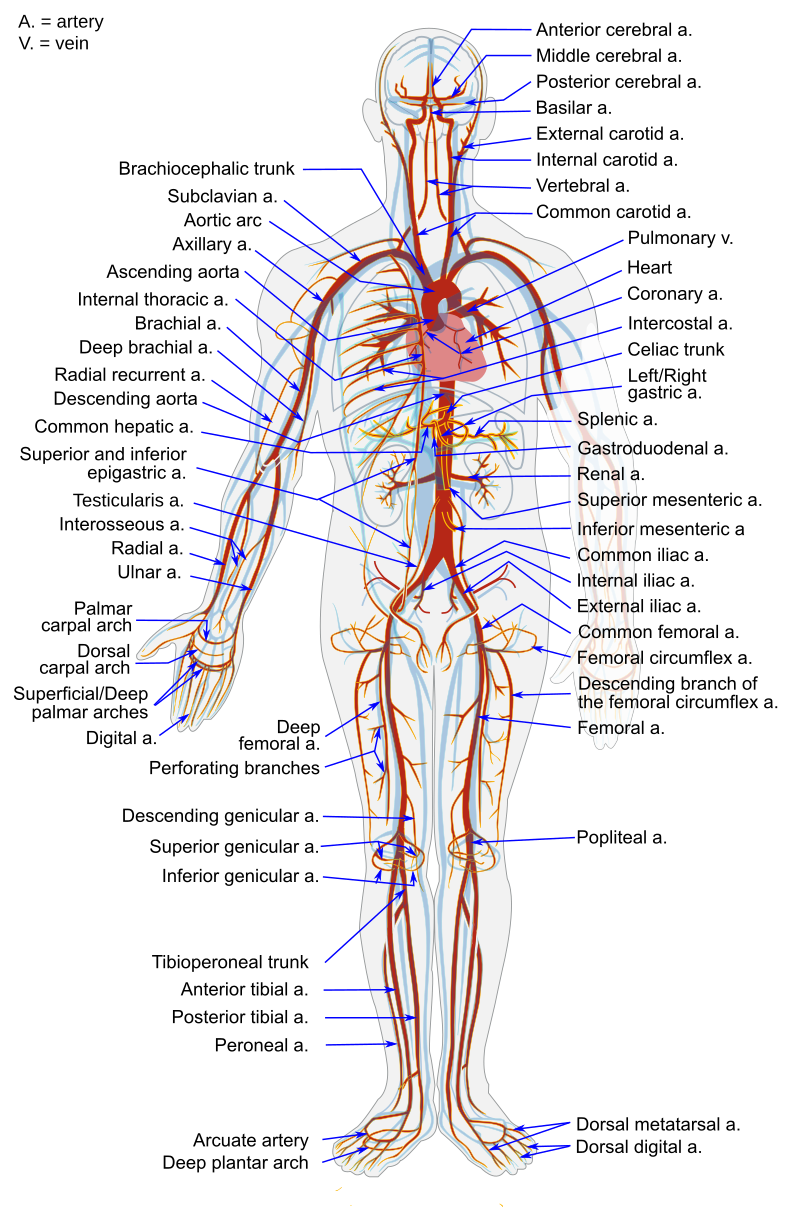
🩸 Major Arteries and Veins - AP Tables
Large blood vessels form the main transport highways of the circulation. Arteries deliver oxygenated blood under high pressure, while veins return deoxygenated blood under low pressure and act as volume reservoirs. Understanding their anatomy and physiology is essential for interpreting cardiovascular disease, imaging, and clinical signs.
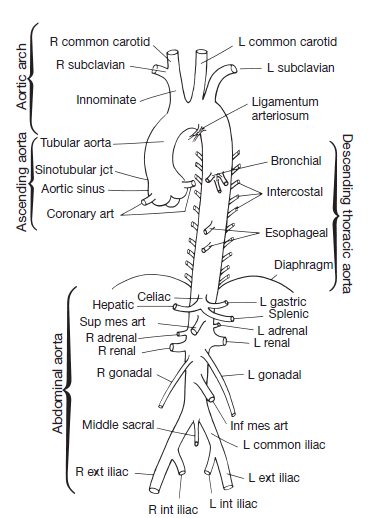
🟥 Table 1 - Major Arteries: AP
| Artery | Origin | Main Supply | Key Anatomical Features | Physiological Role | Clinical Relevance |
|---|---|---|---|---|---|
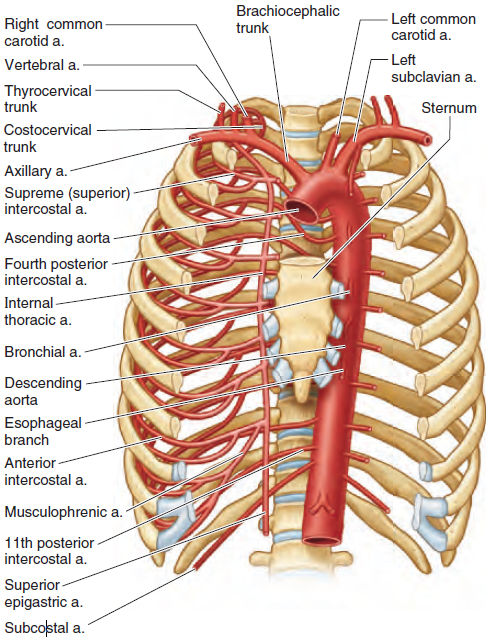
| Aorta | Left ventricle | Entire systemic circulation | Largest elastic artery; arch → thoracic → abdominal | Windkessel effect: maintains diastolic flow | Aneurysm, dissection, coarctation |
| Coronary arteries (LCA, RCA) | Ascending aorta | Heart myocardium | Run on heart surface in grooves | Supply oxygen to cardiac muscle (mainly in diastole) | Ischaemic heart disease, MI |
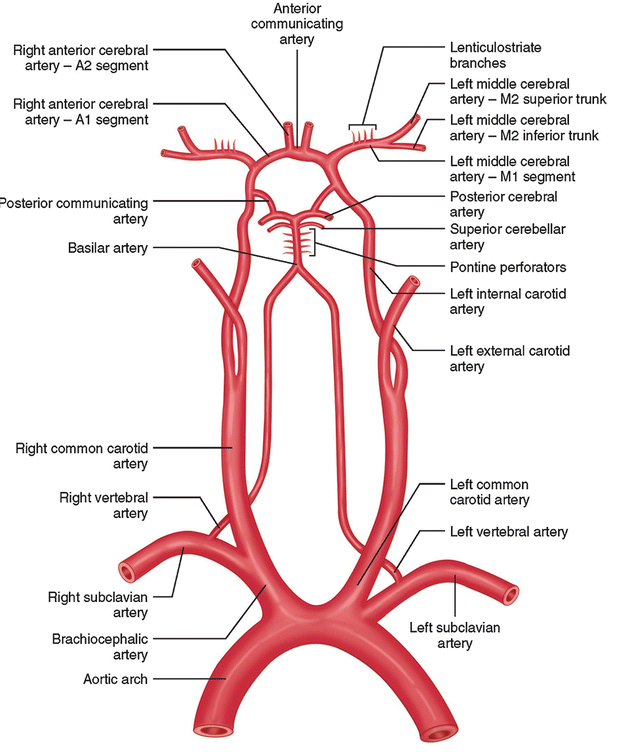
| Common carotid | Aortic arch (L), brachiocephalic (R) | Head and neck | Bifurcates → internal/external carotid | Maintains cerebral perfusion | Stroke, carotid stenosis |
| Internal carotid | Common carotid | Brain, eye | Enters skull via carotid canal | Major cerebral blood supply | TIA, stroke |
| External carotid | Common carotid | Face, scalp, neck | Multiple branches (facial, maxillary) | Supplies superficial tissues | Epistaxis, head/neck surgery |
| Subclavian | Aortic arch / brachiocephalic | Upper limb, brain (via vertebral) | Passes under clavicle | Arm + posterior cerebral flow | Thoracic outlet syndrome |
| Vertebral | Subclavian | Brainstem, cerebellum | Passes through cervical vertebrae | Posterior cerebral circulation | Vertebrobasilar insufficiency |
| Coeliac trunk | Abdominal aorta (T12) | Liver, stomach, spleen | Short trunk → 3 branches | Foregut perfusion | Ischaemia, pancreatitis link |
| Superior mesenteric (SMA) | Abdominal aorta (L1) | Small bowel, proximal colon | Supplies midgut | Intestinal absorption support | Mesenteric ischaemia |
| Inferior mesenteric (IMA) | Abdominal aorta (L3) | Distal colon, rectum | Supplies hindgut | Colonic perfusion | Ischaemic colitis |
| Renal arteries | Abdominal aorta | Kidneys | Short, high-flow vessels | Renal perfusion, BP regulation | Renal artery stenosis |
| Common iliac | Abdominal aorta (L4) | Pelvis, lower limbs | Bifurcates → internal/external | Lower body perfusion | Atherosclerosis |
| Femoral | External iliac | Lower limb | Superficial, palpable | Main leg supply | PAD, catheter access |
| Popliteal | Femoral | Knee, leg | Behind knee joint | Distal limb flow | Popliteal aneurysm |
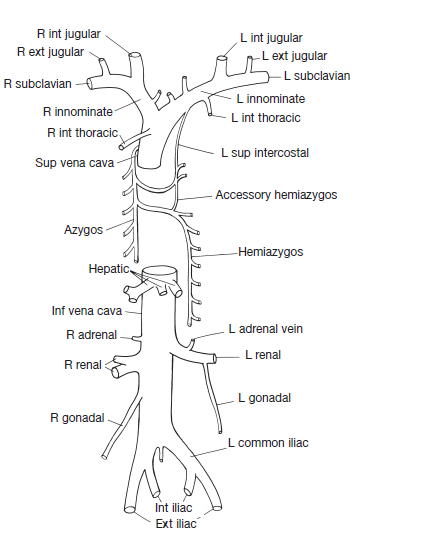
🟦 Table 2 - Major Veins: AP
| Vein | Drains From | Drains Into | Key Anatomical Features | Physiological Role | Clinical Relevance |
|---|---|---|---|---|---|
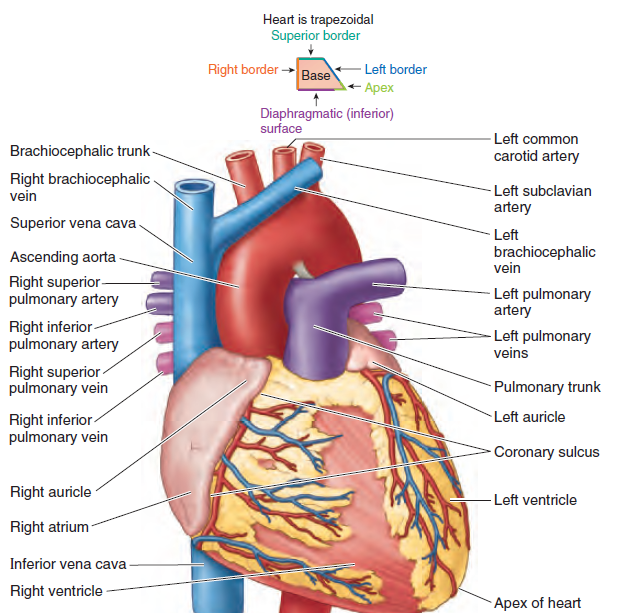
| Superior vena cava (SVC) | Head, neck, upper limbs | Right atrium | Short, wide, no valves | Returns upper body blood | SVC syndrome |
| Inferior vena cava (IVC) | Lower body | Right atrium | Largest vein; retroperitoneal | Main venous return | IVC thrombosis |
| Internal jugular | Brain, face | Brachiocephalic | Runs with carotid artery | Cerebral drainage | Central line access |
| External jugular | Scalp, face | Subclavian | Superficial vein | Surface drainage | Raised JVP sign |
| Brachiocephalic veins | Jugular + subclavian | SVC | Behind sternum | Upper venous return | Thoracic compression |
| Subclavian vein | Upper limb | Brachiocephalic | Under clavicle | Arm drainage | Line insertion risks |
| Portal vein | GI tract, spleen | Liver | Formed by SMV + splenic vein | Nutrient processing | Portal hypertension |
| Hepatic veins | Liver | IVC | Short veins | Drain processed blood | Budd–Chiari syndrome |
| Renal veins | Kidneys | IVC | Left longer than right | Renal drainage | Nutcracker syndrome |
| Common iliac veins | Pelvis, legs | IVC | Behind arteries | Lower body return | May–Thurner syndrome |
| Femoral vein | Lower limb | External iliac | Medial to artery | Deep leg drainage | DVT source |
| Great saphenous vein | Superficial leg | Femoral vein | Longest vein in body | Superficial drainage | Varicose veins, grafting |
| Popliteal vein | Lower leg | Femoral vein | Behind knee | Deep venous return | DVT risk |
| Azygos vein | Thoracic wall | SVC | Right side of spine | Collateral pathway | SVC obstruction bypass |
📝 Integrative Summary
Large arteries act as high-pressure delivery conduits, with elastic vessels smoothing flow and muscular arteries distributing it to organs. Arterioles then determine resistance and tissue perfusion. Large veins act as capacitance vessels, storing most of the circulating blood volume and regulating venous return via valves, muscle pump, and autonomic tone. Most vascular diseases can be understood as problems of: flow (stenosis), pressure (hypertension), volume (heart failure), or integrity (thrombosis/rupture).
📝 Summary
Vascular physiology is the integration of structure (intima–media–adventitia), tone control (endothelium, autonomics, hormones), and haemodynamics (pressure–flow–resistance). Arterioles are the main resistance regulators, capillaries are the main exchange sites, and veins are the main volume reservoirs. Most clinical vascular problems can be framed as failures of tone (shock), wall integrity (atherosclerosis/aneurysm), or fluid balance (oedema).
Major Veins
Other Images
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery