
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - STEMI
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Crib sheets |ECG - LVH |ECG - STEMI |ECG Analysis
Site of Coronary Artery Occlusion in STEMI
- Right coronary artery occlusion
- ST depression in lead I
- ST elevation in lead III greater than in lead II
a. Proximal occlusion- ST elevation more than 1 mm with positive T wave in lead V₄R
b. Distal occlusion- ST isoelectric with a positive T wave in lead V₄R
- Left circumflex artery occlusion
- ST elevation in lead II greater than lead III
- ST isoelectric or elevated in lead I
- ST isoelectric or depressed with negative T wave in V₄R
a. Extension to posterior wall- ST depression in precordial leads
b. Extension to lateral wall- ST elevation in leads I, aVL, V₅, and V₆
- Left anterior descending artery occlusion
a. Proximal to first septal branch and first diagonal branch
- ST elevation in leads aVR and aVL
- ST depression in leads II, III, and aVF
- ST elevation in lead V₁ (> 2 mm) and leads V₂ to V₄
- ST isoelectric or depressed in leads V₅ and V₆
- Acquired intra-Hisian or RBBB may occur
b. Distal to first septal branch, proximal to first diagonal branch- ST elevation in lead I and aVL
- ST depression in lead III (lead II is isoelectric)
- ST elevation in leads V₂ to V₆ but not in lead V₁
c. Distal to first diagonal branch, proximal to first septal branch- ST depression in lead aVL, highest in lead III
- ST elevation in inferior leads, highest in lead III
- ST elevation in leads V₁ to V₄
d. Distal LAD- ST depression in aVR
- ST elevation in inferior leads, highest in lead II
- ST elevation in leads V₃ to V₆
- Left main coronary artery occlusion
- ST elevation in lead aVR
- ST elevation in lead V₁ (lower than that of lead aVR)
- ST depression in leads II and aVF
- ST depression in the precordial leads to the left of V₂

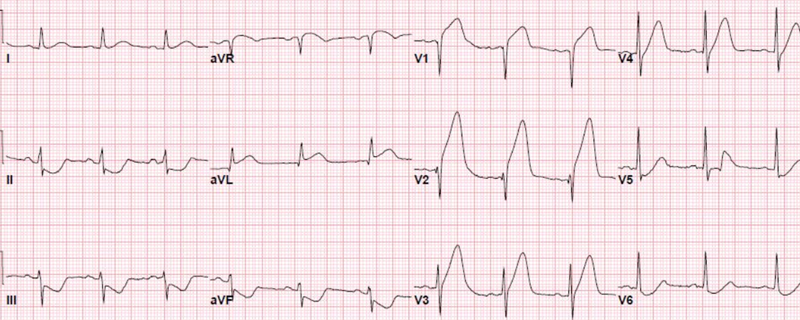
ECG STEMI / MI Patterns: Acute Anterolateral MI
ST ↑ in I, aVL, V3–V6. Poor R wave progression. T wave inversion. Usually LAD occlusion ± RCA/LCx involvement.

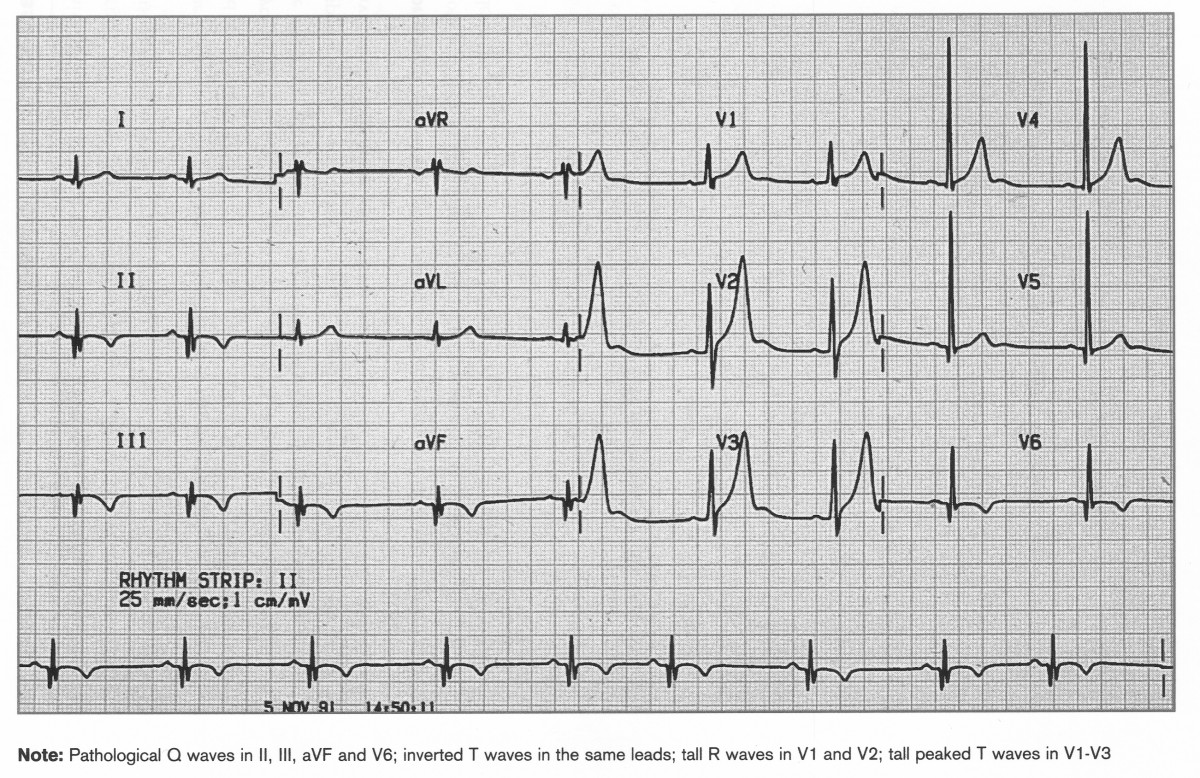
Acute Inferior & Posterior MI
ST ↑ in II, III, aVF. Q waves, T inversion. Posterior MI shows ST ↓ in V1–V2 with tall R in V1. Most often due to RCA occlusion.

Acute Right Ventricular MI
ST ↑ in aVR (± V1). Often accompanies inferior MI. Due to proximal RCA occlusion. Can cause hypotension with nitrates.
Acute Septal MI
ST ↑ in V2–V3. Q waves, T inversion. Due to LAD septal branch occlusion.
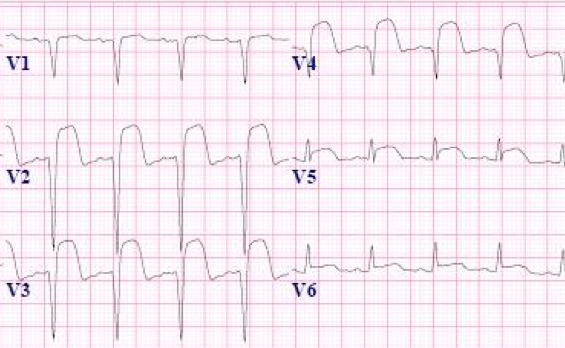
Anterior STEMI with Tombstoning
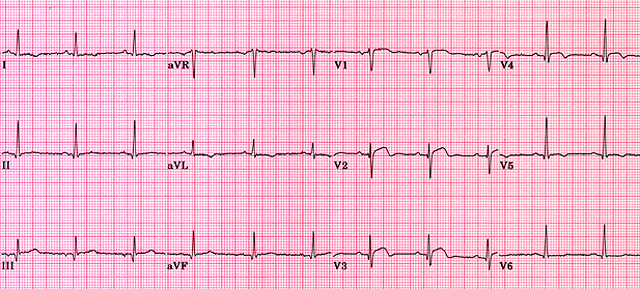
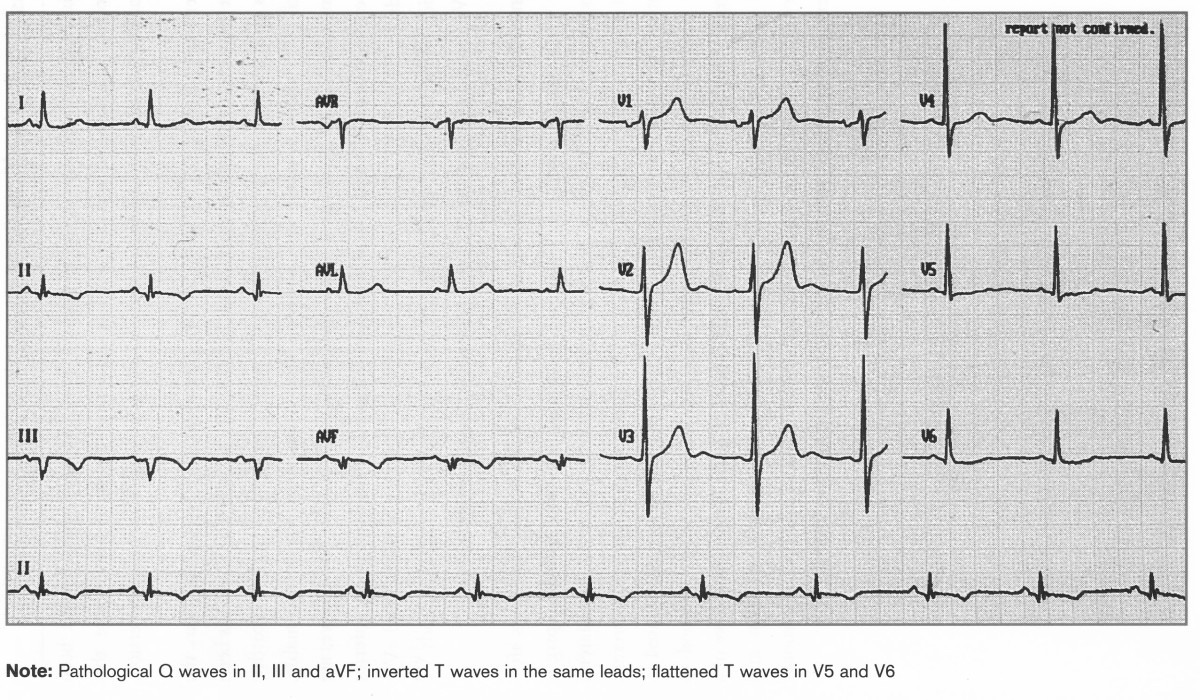
Old Inferior MI
Q waves in II, III, aVF. T inversion/flattening. No acute ST changes.
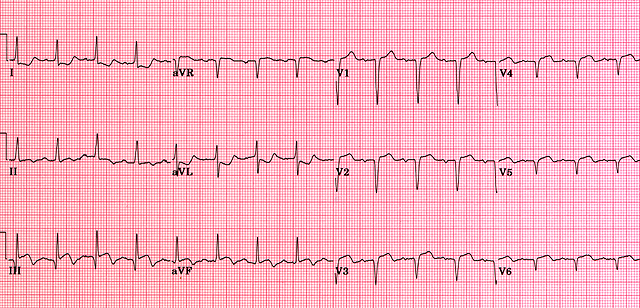
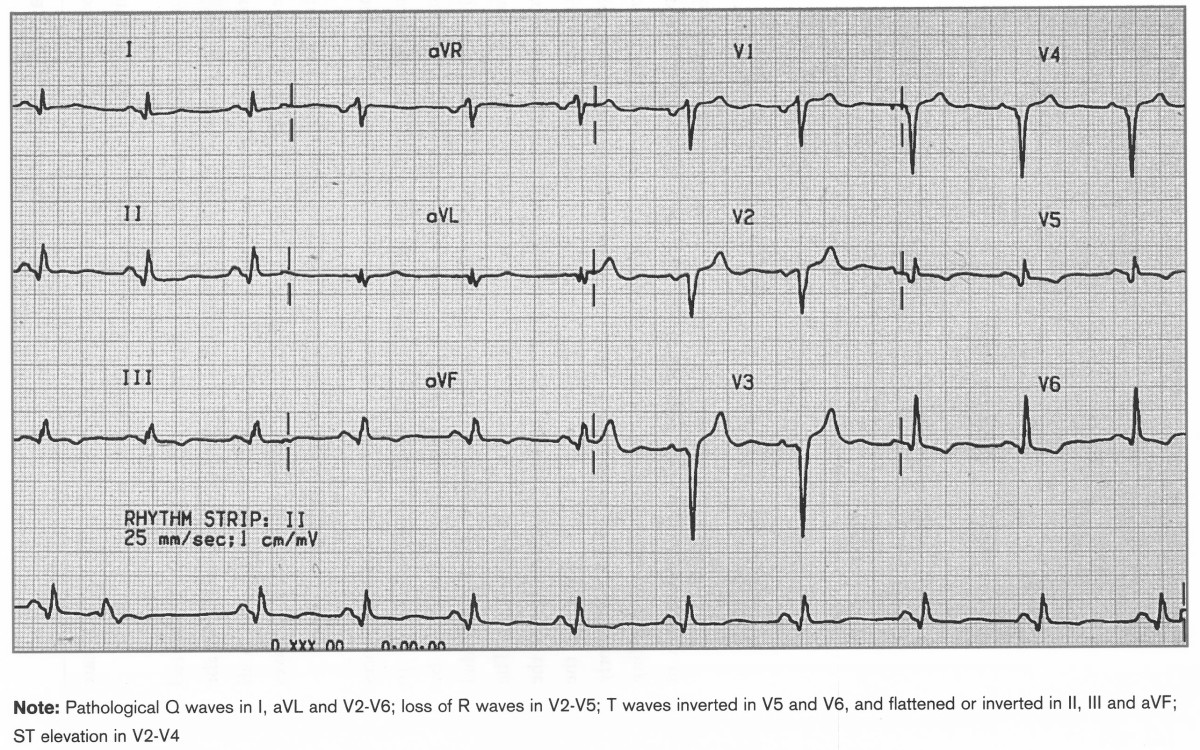
Old Anterolateral MI
Q waves in I, aVL, V2–6. Loss of R waves in V2–5. T inversion V5–V6.
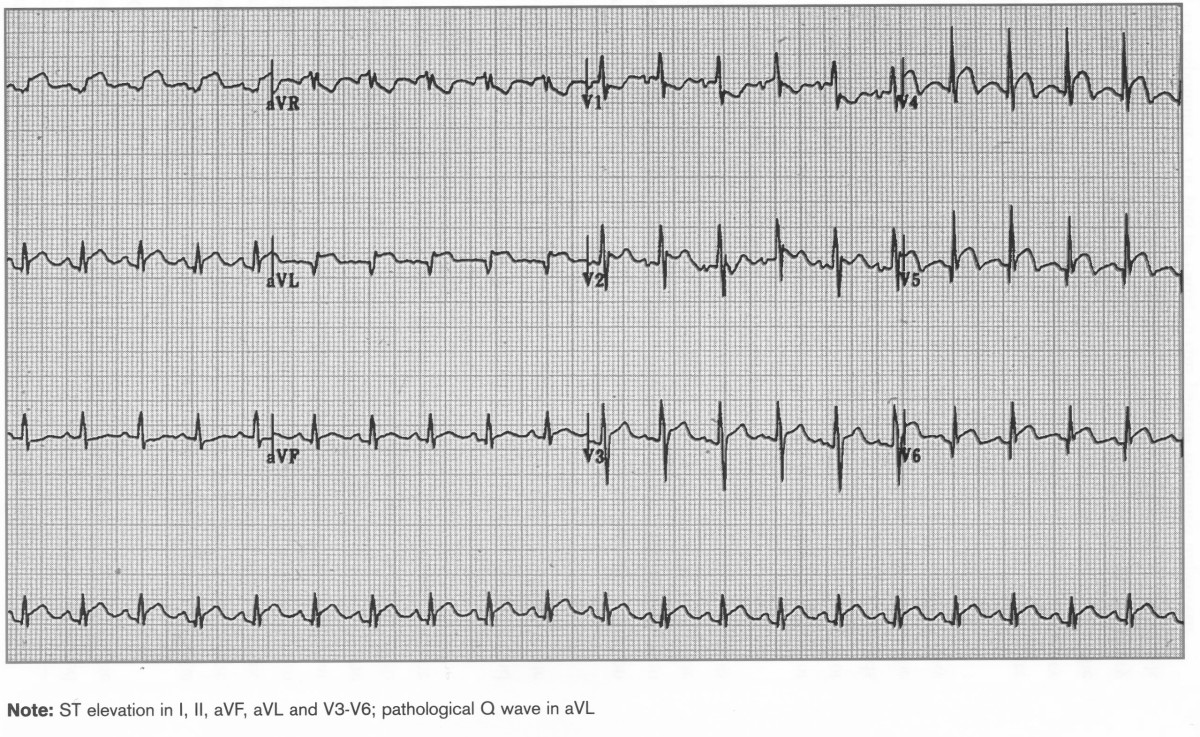
Acute Inferolateral MI
ST ↑ in I, II, aVL, aVF, V3–6. Pathological Q in aVL.
Acute Inf + True Posterior MI
Inferior ST ↑ (II, III, aVF). Posterior changes: ST ↓ V1–V2, tall R in V1.
⚠️ Emergency note: ST elevation + chest pain = treat as STEMI. Activate reperfusion pathway (PCI or thrombolysis) immediately.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery