
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Pathological Gaits 🚶♂️
Gait is a dynamic neurological examination that integrates cortex, basal ganglia, cerebellum, brainstem, spinal cord, peripheral nerves, and muscle. Abnormal gait patterns often provide earlier and more reliable localisation than isolated power testing. In clinical practice and UK exams, recognising the gait pattern is usually more important than naming the disease.
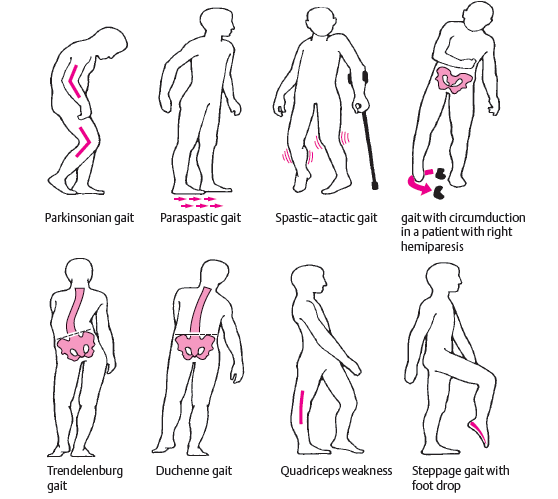
🧠 Hemiplegic (Circumduction) Gait
This gait is caused by unilateral upper motor neuron weakness, most commonly following stroke. The affected leg is stiff and extended, swinging outward in a semicircle to clear the ground due to spasticity and reduced knee flexion. The ipsilateral arm is typically flexed and adducted.
- Cause: Corticospinal tract lesion above decussation
- Features: Stiff leg, circumduction, reduced arm swing
- Think: Stroke, brain tumour, MS, demyelination
🧠 Spastic Diplegic (Scissoring) Gait
Spasticity predominantly affects both legs, leading to hip adduction and crossing of the legs during walking. This reflects bilateral corticospinal tract involvement, often with relative sparing of the arms.
- Cause: Bilateral UMN pathology
- Features: Narrow base, legs crossing (“scissoring”)
- Think: Cerebral palsy, cervical myelopathy
🧠 Parkinsonian Gait
Parkinsonian gait reflects basal ganglia dysfunction with impaired initiation and scaling of movement. Patients walk with short, shuffling steps, reduced arm swing, and a stooped posture. Festinating gait may develop, where steps become progressively faster and shorter.
- Cause: Dopaminergic deficit in basal ganglia circuits
- Features: Shuffling, freezing, reduced arm swing
- Think: Parkinson’s disease, drug-induced parkinsonism
🎯 Cerebellar Ataxic Gait
Cerebellar disease produces a wide-based, unsteady gait with irregular steps and truncal instability. Patients appear “drunk” and may veer to one side. Visual input does not significantly improve stability, distinguishing it from sensory ataxia.
- Cause: Cerebellar hemisphere or vermis pathology
- Features: Wide base, staggering, poor tandem gait
- Think: Alcohol-related disease, stroke, tumour
🦵 Sensory Ataxic (Stamping) Gait
Loss of proprioception leads patients to rely heavily on visual input for balance. They walk with high-stepping, forceful foot placement and become markedly worse in the dark or with eyes closed. This is classically associated with a positive Romberg’s test.
- Cause: Dorsal column or peripheral nerve disease
- Features: Stamping gait, worse without visual input
- Think: Vitamin B12 deficiency, peripheral neuropathy
💪 Myopathic (Waddling) Gait
Proximal muscle weakness, particularly of the hip girdle, causes instability during single-leg stance. Patients compensate by tilting their trunk side-to-side, producing a waddling appearance. Rising from a chair or climbing stairs is often difficult.
- Cause: Proximal muscle weakness
- Features: Waddling, lordosis, difficulty standing
- Think: Muscular dystrophy, inflammatory myopathy
⚡ High-Stepping (Foot Drop) Gait
Weak ankle dorsiflexion causes the foot to drag during swing phase. Patients compensate by lifting the knee higher than normal to avoid tripping. The foot often slaps the ground on contact.
- Cause: Common peroneal nerve or L5 root lesion
- Features: High knee lift, foot slap
- Think: Peripheral neuropathy, radiculopathy
🧠 Frontal (Apraxic) Gait
Despite preserved strength, patients struggle to initiate walking and take short, hesitant steps. The gait appears “magnetic,” as if the feet are stuck to the floor. This reflects impaired motor planning rather than weakness.
- Cause: Frontal lobe or subcortical disease
- Features: Difficulty initiating gait, short steps
- Think: Normal pressure hydrocephalus, vascular dementia
🩺 Teaching Pearl
When assessing gait, ask: is the base wide or narrow, are the steps symmetric, and does vision help? Answering these three questions will usually localise the problem before you even test power. Gait is one of the highest-yield parts of the neurological examination.
🚶♂️ Pathological Gaits – Clinical Localisation Table
| Gait Pattern | Key Features | Likely Lesion | Typical Causes |
|---|---|---|---|
| Hemiplegic (Circumduction) | Stiff extended leg, swings outward; flexed adducted arm | Unilateral corticospinal tract (UMN) | Stroke, brain tumour, demyelination |
| Spastic Diplegic (Scissoring) | Narrow base, legs cross, increased tone | Bilateral corticospinal tracts | Cerebral palsy, cervical myelopathy |
| Parkinsonian | Shuffling steps, reduced arm swing, freezing, festination | Basal ganglia (dopaminergic pathways) | Parkinson’s disease, drug-induced parkinsonism |
| Cerebellar Ataxic | Wide-based, staggering, poor tandem gait | Cerebellum (vermis or hemispheres) | Alcohol-related disease, stroke, tumour |
| Sensory Ataxic (Stamping) | High-stepping, forceful foot placement, worse in dark | Dorsal columns / peripheral nerves | Vitamin B12 deficiency, neuropathy |
| Myopathic (Waddling) | Side-to-side trunk sway, difficulty standing | Proximal muscles (hip girdle) | Muscular dystrophy, inflammatory myopathy |
| High-Stepping (Foot Drop) | Excessive knee lift, foot slap | Peroneal nerve / L5 root | Peripheral neuropathy, radiculopathy |
| Frontal (Apraxic / Magnetic) | Difficulty initiating gait, short hesitant steps | Frontal lobes / subcortical circuits | Normal pressure hydrocephalus, vascular dementia |
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery