
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Renal Tubular Acidosis (RTA)
Related Subjects: |Metabolic acidosis |Aspirin or Salicylates toxicity |Ethylene glycol toxicity |Renal Tubular Acidosis |Lactic acidosis
🧪 Renal Tubular Acidosis (RTA) is characterized by the inability of the kidneys to excrete acidic urine, leading to a persistently high urinary pH >5.5 even under an acid load. It results in a normal anion gap (hyperchloremic) metabolic acidosis due to failure of renal acid excretion.
ℹ️ About
- The body is a net acid producer from metabolism (≈1 mmol/kg/day H⁺ ions).
- Normal plasma is slightly alkaline (pH ~7.40), while urine is normally acidic (pH 5–6).
- RTA arises from failure of the tubules to handle H⁺ or HCO₃⁻ appropriately.
🧬 Aetiology
- Defects in tubular transport mechanisms.
- Failure in:
- Distal tubule H⁺ secretion (distal RTA).
- Proximal tubule HCO₃⁻ reabsorption (proximal RTA).
- Leads to normal anion gap (hyperchloremic) metabolic acidosis.
📑 Types of RTA
- Type 1 (Distal RTA): Failure to excrete H⁺ ions → urine cannot be acidified.
- Type 2 (Proximal RTA): Failure to reabsorb HCO₃⁻.
- Type 3: Rare, mixed features of Types 1 & 2.
- Type 4: Hypoaldosteronism/hyporeninaemia → impaired H⁺ & K⁺ excretion → hyperkalemic RTA.
| Type | Defect | Associations | Key Management |
|---|---|---|---|
| 1 (Distal) | Failure to excrete H⁺ (↓ urine acidification) | SLE, Sjögren’s, sickle cell, Ehlers-Danlos, autoimmune disease, toxins (Toluene, Lithium, Amphotericin) | Oral bicarbonate; prevent renal stones |
| 2 (Proximal) | Failure to reabsorb HCO₃⁻ | Fanconi syndrome, Wilson’s disease, amyloidosis, myeloma | Oral bicarbonate ± Vitamin D; phosphate replacement |
| 3 (Mixed) | Features of Type 1 + 2 (rare) | Renal insufficiency | Treat underlying cause |
| 4 (Hyperkalemic) | Reduced aldosterone effect → ↓ H⁺ & K⁺ excretion | Diabetes, interstitial nephritis, ACEi/ARB, NSAIDs, K-sparing diuretics | Fludrocortisone, loop/thiazide diuretics, K⁺ binders, bicarbonate |
🩺 Clinical Features
- Type 1: Growth delay, nephrolithiasis, nephrocalcinosis, polydipsia, muscle weakness.
- Type 2: Growth delay, rickets/osteomalacia, Fanconi syndrome (glycosuria, aminoaciduria, phosphate wasting).
- Type 4: Often asymptomatic; may present with hyperkalemia in diabetics or interstitial nephritis.
🔎 Investigations
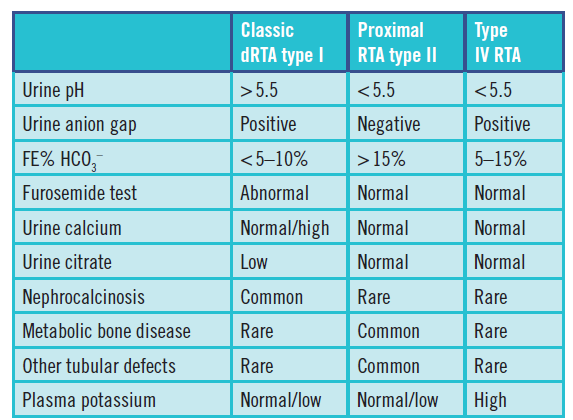
- U&E: Hypokalaemia (Types 1 & 2), Hyperkalaemia (Type 4).
- VBG: Normal anion gap metabolic acidosis (hyperchloremic).
- Urine pH: >5.5 in Type 1 (inability to acidify), variable in Type 2, normal/low in Type 4.
🧪 Diagnostic Tests
- Type 1: NaHCO₃ infusion → failure to generate urine–blood pCO₂ gradient.
- Type 2: NaHCO₃ loading test; check for Fanconi features.
- Type 4: NH₄⁺ loading test; confirms impaired distal acidification.
💊 Management
- Alkali therapy (oral bicarbonate or citrate) for Types 1 & 2.
- Potassium supplementation for hypokalaemic patients (Types 1 & 2).
- Vitamin D and phosphate for osteomalacia/rickets (Type 2).
- For Type 4: fludrocortisone (if hypoaldosteronism), loop/thiazide diuretics, potassium binders, alkali therapy.
💡 Exam Pearls:
• RTA = normal anion gap metabolic acidosis (hyperchloremic).
• Type 1 → renal stones/nephrocalcinosis, urine pH >5.5.
• Type 2 → Fanconi features, phosphate wasting.
• Type 4 → hyperkalaemia, common in diabetics on ACEi/ARB.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery