
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Anatomy and Physiology of the Large Bowel (Colon, Rectum, Anal Canal)
Related Subjects: |AP of the Oesophagus |AP of the Diaphragm |AP of the Large Bowel (Colon, Rectum, Anal Canal) |AP of Small Bowel |AP of the Biliary system |AP of the Bone Marrow |AP of the Eye |AP of the Pharynx |AP of the Larynx |AP of the Ear |AP of the Nose |AP of Male Genitalia |AP of the Breast |AP of the Stomach |AP of the Rectum |AP of the Spleen
The large bowel extends from the ileocaecal valve to the anus and is specialised for water and electrolyte absorption, microbial fermentation, and formation, storage, and controlled elimination of faeces. Anatomically it is identified by taeniae coli (3 longitudinal muscle bands), haustra (sacculations), and epiploic appendages (fat tags). Function depends on coordinated motility patterns (haustral “mixing” and mass movements), an intact mucosal barrier, and a complex enteric–autonomic control system.
🏗️ Gross Anatomy: Parts of the Large Bowel
- Caecum: First part, typically in the right iliac fossa. Receives chyme from ileum via the ileocaecal valve, which helps regulate entry and limits reflux back into ileum.
- Appendix: Worm-like blind-ended tube arising from the caecum; rich in lymphoid tissue (GALT) with immune and microbiome “reservoir” roles proposed.
📌 Clinical: acute appendicitis; position varies (retrocaecal common) affecting pain pattern. - Ascending colon: Runs superiorly on the right → hepatic flexure near the liver.
- Transverse colon: Crosses abdomen right → left to splenic flexure near spleen; highly mobile due to transverse mesocolon. 🌀
- Descending colon: Runs down the left abdomen → sigmoid colon.
- Sigmoid colon: S-shaped segment in left iliac fossa/pelvis; major role in storage and propulsion into rectum.
📌 Clinical: common site for diverticulosis/diverticulitis; common site for volvulus in predisposed anatomy. - Rectum: Pelvic reservoir for faeces; follows sacral curvature; ends at the anorectal junction.
- Anal canal & anus: Terminal segment with specialised continence mechanisms:
- Internal anal sphincter = involuntary smooth muscle (continuation of circular layer).
- External anal sphincter = voluntary skeletal muscle (pudendal nerve control) working with pelvic floor.
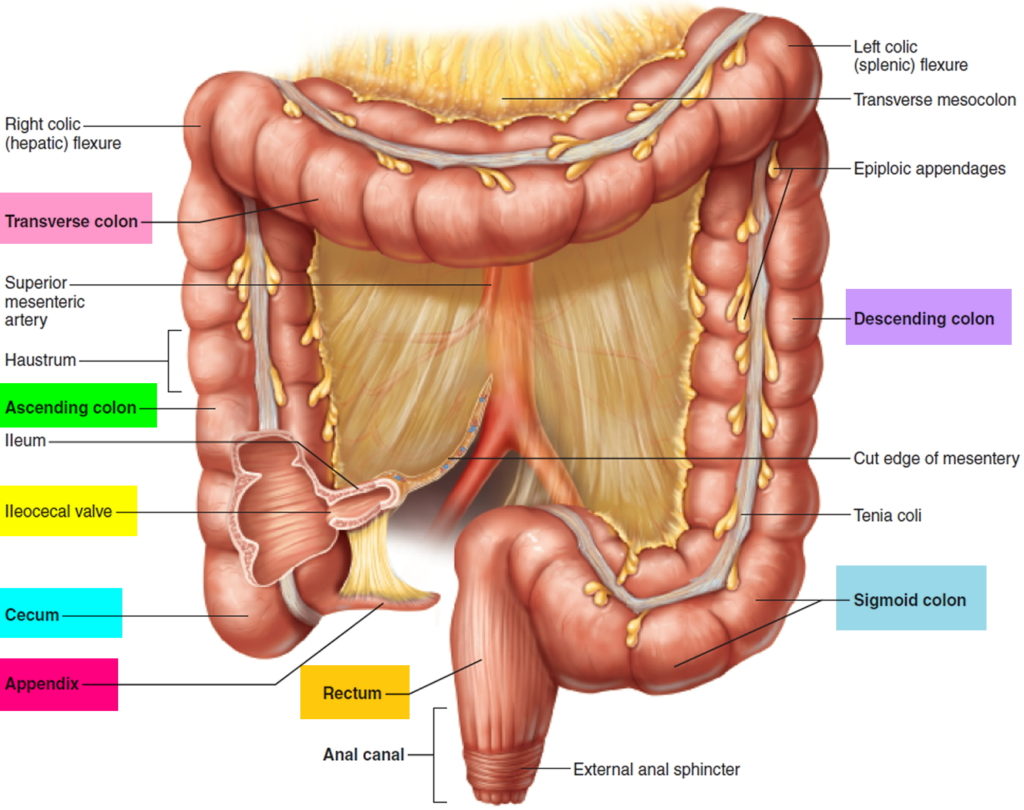
🧩 Key Structural Features (How to recognise colon)
- Taeniae coli (3 bands): longitudinal muscle condensed into three ribbons; converge at the appendix base (useful landmark in surgery).
- Haustra: sacculations created by taeniae shortening relative to the colon wall; allow mixing and slow transit.
- Epiploic appendages: fat-filled peritoneal outpouchings; can infarct (epiploic appendagitis) mimicking diverticulitis/appendicitis.
- Mucosa: no villi (unlike small bowel); dense straight crypts with many goblet cells → mucus lubrication/protection.
📍 Peritoneal Relationships & Mobility
- Intraperitoneal: transverse colon and sigmoid colon (mobile; mesocolon present).
- Secondarily retroperitoneal: ascending and descending colon (more fixed).
- Clinical: mobility influences pain localisation, volvulus risk (sigmoid), and surgical access.
⚙️ Physiology of the Large Intestine
The large intestine is essential for 💧 water & electrolyte absorption, 🦠 bacterial fermentation of fibre, 💩 faeces formation and storage, and 🛡️ mucosal immune defence. It turns liquid ileal effluent into formed stool while preserving fluid balance.
🔑 Core Functions (with mechanisms)
- 💧 Water & electrolyte absorption:
- Absorbs Na⁺ (active) and Cl⁻ (often coupled), with water following osmotically.
- Aldosterone increases distal colonic Na⁺ absorption and K⁺ secretion (important in diarrhoeal states and electrolyte loss).
- Colon can “salvage” fluid-when overwhelmed (infection, inflammation, osmotic load), diarrhoea results.
- 🦠 Microbiota fermentation:
- Fibre (non-digestible carbohydrates) is fermented → short-chain fatty acids (SCFAs): acetate, propionate, butyrate.
- Butyrate is a major fuel for colonocytes and supports mucosal integrity; SCFAs also promote sodium/water absorption and influence metabolic signalling.
- Gas production (H₂, CO₂, methane) contributes to bloating and flatus.
- 💩 Stool formation & storage:
- Progressive dehydration + mixing → formed stool.
- Rectum acts as a reservoir; sensation of fullness depends on rectal wall stretch and compliance.
- 🧴 Mucus secretion:
- Goblet cell mucus lubricates stool and forms a protective layer separating bacteria from epithelium.
- Protection becomes critical during inflammation (e.g., colitis) where barrier disruption increases symptoms and bleeding risk.
- 🛡️ Immune function:
- Large bowel contains extensive GALT, innate immune cells, and IgA responses-maintaining tolerance to commensals while responding to pathogens.
- Dysbiosis and immune dysregulation contribute to IBD pathophysiology.
🌊 Motility Patterns (How the colon moves)
Colonic motility balances slow mixing (to maximise absorption) with periodic propulsive events (to advance contents). The enteric nervous system coordinates local reflexes, while autonomic input modulates overall tone and sphincter control.
- Haustral (segmental) contractions: rhythmic mixing movements that churn contents and expose them to mucosa for absorption.
- Mass movements: powerful, longer-range peristaltic waves that propel stool toward rectum, often occurring after meals (gastrocolic reflex).
- Rectosigmoid “brake”: functional slowing at rectosigmoid junction helps maintain continence by limiting constant rectal filling.
🚽 Defecation (Reflex + Voluntary Control)
Defecation integrates a spinal reflex (parasympathetic) with voluntary control (pudendal nerve) and pelvic floor mechanics. Continence depends on anal sphincters, rectal compliance, and the anorectal angle maintained by the puborectalis sling.
- 📈 Rectal distension: stretch receptors trigger the defecation reflex.
- 🚪 Internal anal sphincter relaxation (involuntary):
- Rectal distension causes reflex relaxation of the internal sphincter (rectoanal inhibitory reflex) allowing “sampling” of rectal contents.
- Distinguishing gas vs liquid vs solid helps decide whether to defecate.
- 🧠 External sphincter + pelvic floor (voluntary):
- External sphincter and puborectalis contract to delay defecation; relaxation straightens the anorectal angle to permit passage.
- Valsalva and abdominal wall contraction raise intra-abdominal pressure to assist expulsion.
- 🌊 Propulsion: mass movement + rectal contraction + sphincter relaxation = stool expulsion.
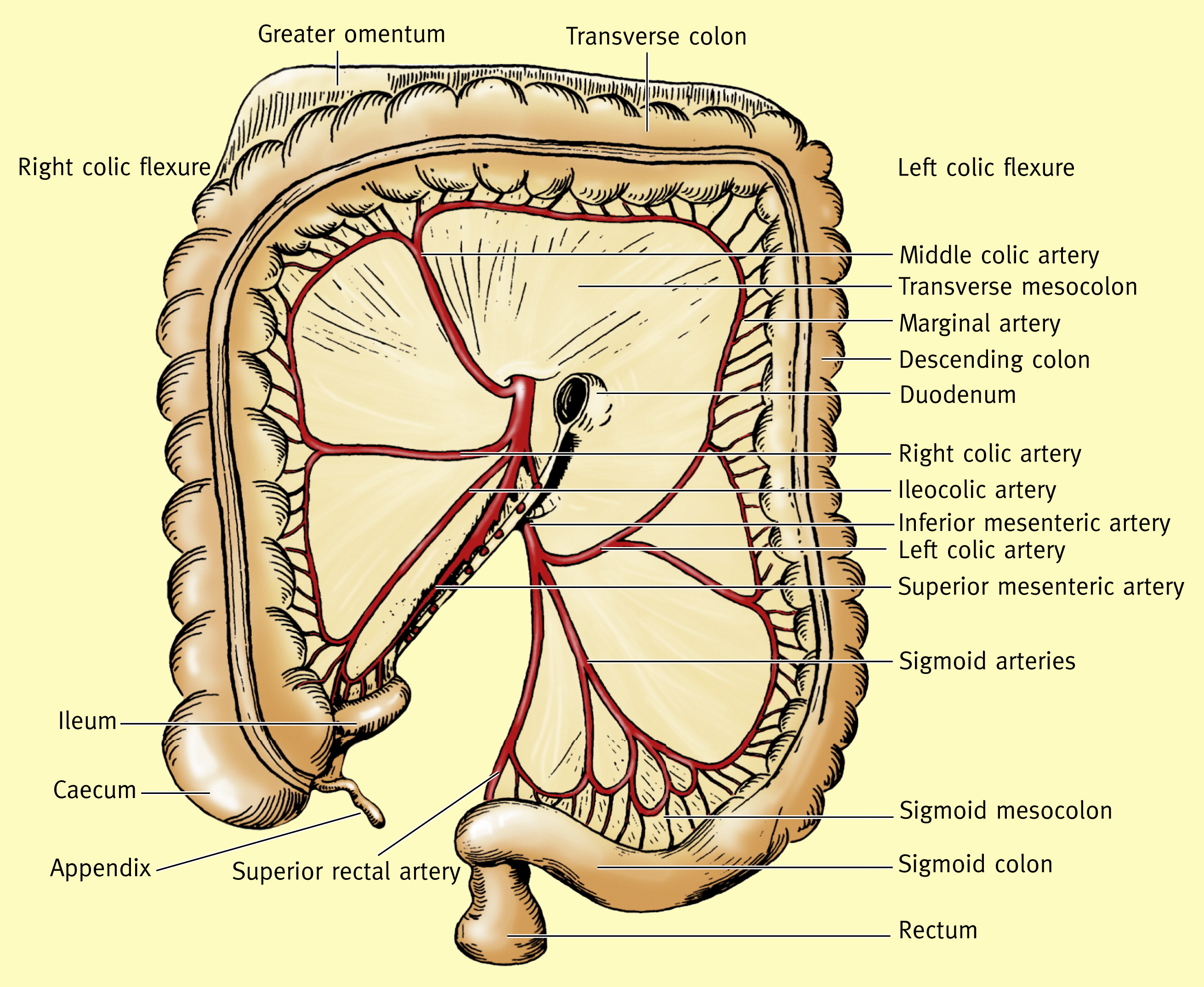
🩸 Blood Supply (Arterial, Venous, Watershed Areas)
- Arterial supply:
- SMA territory: caecum → ascending colon → proximal 2/3 of transverse colon.
- IMA territory: distal 1/3 transverse colon → descending → sigmoid → upper rectum.
- Rectum:
- Superior rectal (from IMA) supplies upper rectum.
- Middle rectal (internal iliac) and inferior rectal (internal pudendal) supply mid/lower rectum and anal canal.
- Marginal artery (of Drummond): an anastomotic arcade along the colon linking SMA and IMA territories (variable robustness).
- Watershed zones (ischaemia risk):
- Splenic flexure (Griffiths’ point): SMA–IMA border zone.
- Rectosigmoid junction (Sudeck’s point): IMA–rectal supply transition.
- Venous drainage:
- SMV + IMV → portal vein → liver.
- Anal canal has systemic–portal connections (relevant to haemorrhoids and portal hypertension patterns).
🧠 Nerve Supply (Enteric + Autonomic)
- Enteric nervous system: intrinsic control via myenteric (motility) and submucosal (secretion/blood flow) plexuses.
- Parasympathetic (↑ motility & secretion):
- Vagus nerve: proximal colon (to splenic flexure).
- Pelvic splanchnic nerves (S2–S4): distal colon, rectum, anal canal.
📌 Crucial for the defecation reflex.
- Sympathetic (↓ motility, ↑ sphincter tone):
- Via superior and inferior mesenteric plexuses → reduces motility/secretion, contracts internal sphincter, and modulates blood flow.
- Somatic control (continence):
- Pudendal nerve controls external anal sphincter and pelvic floor (voluntary continence).
🧪 Histology: What makes colon different?
- No villi; long straight crypts (crypts of Lieberkühn).
- Many goblet cells → mucus lubrication and barrier maintenance.
- Absorptive colonocytes with tight junctions regulate water/electrolyte transport.
- Immune cells within lamina propria support pathogen defence and tolerance.
⚠️ Clinical Relevance
- 🚫 Constipation: slow transit → excessive water absorption → hard stools; can be due to low fibre, immobility, opioids, metabolic causes.
- 💦 Diarrhoea: rapid transit and/or secretion/inflammation → reduced absorption; risks dehydration and electrolyte disturbance.
- 🔥 Diverticular disease: outpouchings (often sigmoid) related to wall weakness and pressure; diverticulitis causes LLQ pain, fever, altered bowel habit.
- 🎗️ Colorectal cancer: common; right-sided lesions may present with iron deficiency/occult bleeding, left-sided lesions with change in bowel habit/obstruction.
- 🩸 Ischaemic colitis: classically affects watershed zones (splenic flexure, rectosigmoid) after hypotension/vascular disease → crampy pain + rectal bleeding.
- 🧠 IBD: ulcerative colitis (continuous colonic mucosal inflammation) vs Crohn’s (transmural, skip lesions) → diarrhoea, pain, bleeding, systemic effects.
📊 Quick Teaching Table
| Section | Key Feature | Blood Supply | High-yield Clinical Note |
|---|---|---|---|
| Caecum | Ileocecal valve + appendix base landmark | SMA | Appendicitis; caecal volvulus (less common) |
| Ascending | Right colon → hepatic flexure | SMA | Right-sided cancer → occult bleeding/IDA |
| Transverse | Mobile; long segment | SMA (prox 2/3), IMA (dist 1/3) | Border-zone perfusion; mesocolon mobility |
| Descending | Left colon; more fixed | IMA | Splenic flexure nearby = watershed ischaemia risk |
| Sigmoid | Storage + propulsion into rectum | IMA | Diverticulitis common; sigmoid volvulus risk |
| Rectum | Reservoir; compliance important | Sup rectal (IMA) + iliac branches | Cancer; haemorrhoids; proctitis |
| Anal canal | Continence zone; sphincters + pelvic floor | Inf rectal (pudendal) + others | Fissures, haemorrhoids; important sensory differences above/below dentate line |
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery