
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Pericardial Effusion and Tamponade ✅
Related Subjects: | Assessing Breathlessness | Acute Hypotension | Respiratory Failure | Pulmonary Embolism | Deep Vein Thrombosis | DVT/PE in Pregnancy | CTPA
💉 Cardiac tamponade is a medical emergency where rising intrapericardial pressure impairs ventricular filling → ↓ stroke volume → ↓ cardiac output → obstructive shock and cardiac arrest 🚨. 👉 Classic Beck’s triad: ↑ JVP, hypotension, muffled heart sounds (often incomplete in practice). 👉 Immediate pericardial decompression is life-saving - do NOT delay for imaging if unstable. 🩺 Point-of-care echocardiography confirms diagnosis (RA/RV diastolic collapse). ⚡ Emergency options: ultrasound-guided pericardiocentesis (first-line) or surgical drainage.
📖 Overview of Pericardial Effusion
- 💧 Pericardial effusion = fluid accumulation (serous, blood 🩸, pus 🦠, chyle).
- ⚖️ Normal volume: 10–50 mL
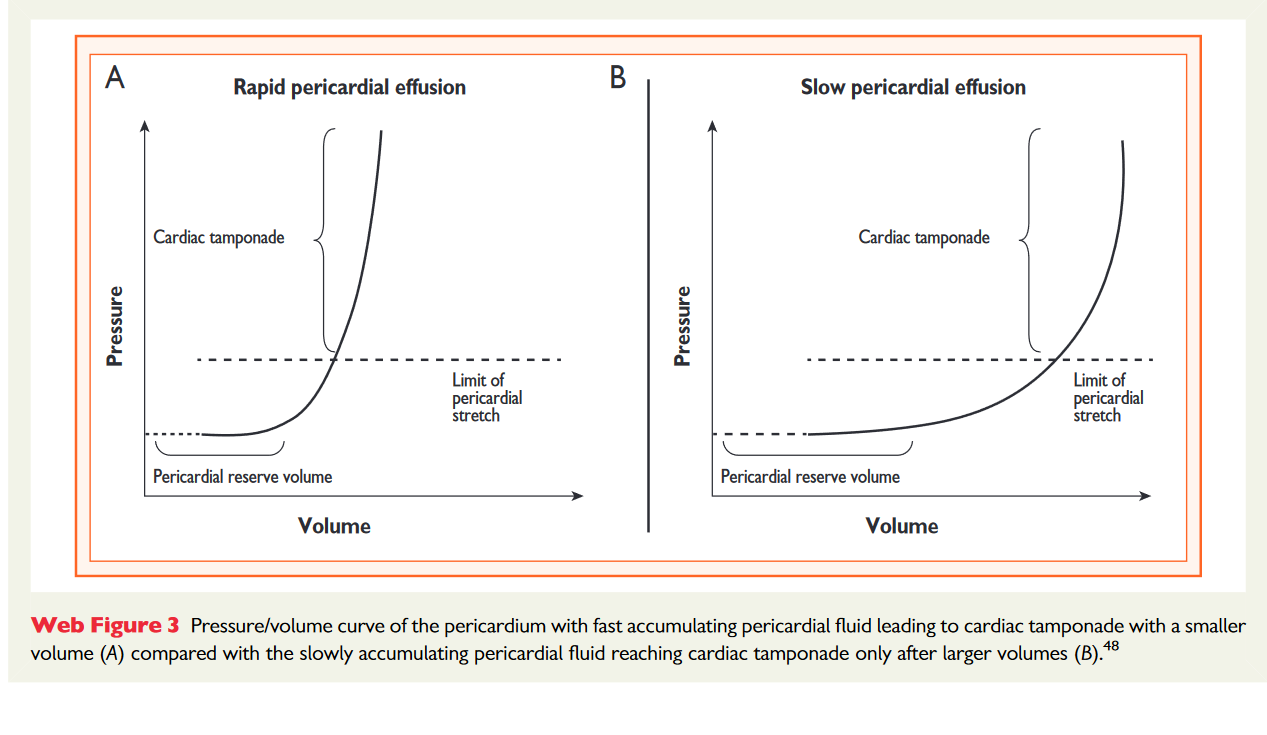
- 📈 Slow accumulation → pericardium stretches → large volumes tolerated
- ⚡ Rapid accumulation (even 100–200 mL) → sharp pressure rise → tamponade
- 🧠 Key concept: rate of accumulation matters more than absolute volume
🩺 Aetiology
- 🦠 Infective: Viral (commonest), TB (important globally), bacterial
- 🔥 Autoimmune: SLE, RA, vasculitis
- 🎗️ Malignancy: Lung, breast, lymphoma, melanoma
- 💔 Post-cardiac injury: MI (Dressler’s), surgery, trauma
- 🧪 Metabolic: Uraemia, hypothyroidism
- 🩸 Vascular: Aortic dissection, free wall rupture post-MI
- 💊 Iatrogenic: Anticoagulation → haemopericardium
📊 Classification
- ⏱️ Time: Acute / Subacute (<3 months) / Chronic (>3 months)
- 📐 Size (echo): Mild (<10 mm), Moderate (10–20 mm), Large (>20 mm)
- 🫀 Haemodynamic: No compromise / Tamponade / Effusive-constrictive
- 📍 Distribution: Circumferential vs loculated
⚠️ Causes of Tamponade (High-Yield)
- 🚑 Trauma or iatrogenic (procedures, pacing wires)
- 🎗️ Malignancy (common cause of large effusions)
- 🦠 TB (important in endemic populations)
- 🩸 Aortic dissection (life-threatening cause)
- 💔 Post-MI free wall rupture (3–10 days)
- 💊 Anticoagulation → haemopericardium
👩⚕️ Clinical Features (Effusion without Tamponade)
- Dyspnoea, fatigue, chest discomfort
- Orthopnoea, PND
- Systemic features: fever, weight loss (TB/malignancy)
- Pressure effects: dysphagia, hoarseness
💡 Pulsus paradoxus = inspiratory drop in SBP >10 mmHg (mechanism: ↑ RV filling → septal shift → ↓ LV filling)
⚠️ Always consider life-threatening differentials: PE, ACS/MI, Type A aortic dissection, tension pneumothorax
🚨 Clinical Features of Cardiac Tamponade
- Severe dyspnoea, tachycardia, hypotension → shock
- Beck’s triad:
- ↑ JVP
- ↓ BP
- 🔇 Muffled heart sounds
- ❗ Narrow pulse pressure
- ❗ Tachycardia almost universal
- ❗ Absent Y descent (distinguishes from constriction)
🔎 Investigations
- ECG: Sinus tachycardia, low voltage, electrical alternans
- CXR: “Water bottle” heart (large chronic effusion)
- Echo (GOLD STANDARD):
- RA/RV diastolic collapse 🚨
- Dilated non-collapsing IVC
- Swinging heart
- Bloods: FBC, CRP, U&E, TFTs, troponin
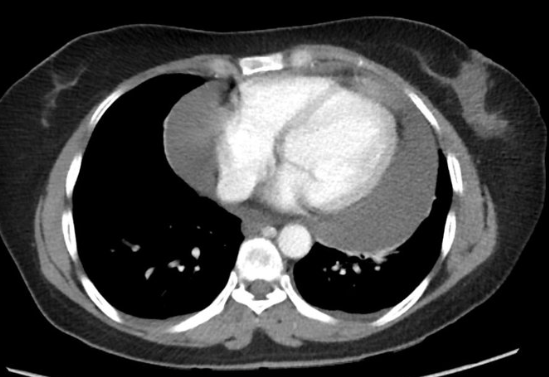
- CT/MRI: For complex/loculated effusions
- Pericardial fluid analysis: Cytology, culture, TB PCR
💊 Management (Guideline-Aligned)
🚨 Tamponade = IMMEDIATE DRAINAGE Do NOT delay for definitive diagnosis if unstable.
- 🅰️ ABC approach + oxygen
- 💧 IV fluids → temporising (↑ preload)
- 🩺 Urgent pericardiocentesis (ultrasound-guided) = first-line
- 🔪 Surgical drainage if traumatic, recurrent, or loculated
- ❗ Leave drain in situ to prevent re-accumulation
- 💊 Cause-specific treatment:
- NSAIDs + colchicine → inflammatory pericarditis
- Dialysis → uraemic
- Oncology input → malignant
- Anti-TB therapy → tuberculous
⚠️ Avoid:
- ❌ Diuretics (↓ preload → worsens tamponade)
- ❌ Positive pressure ventilation (↓ venous return)
- ❌ Delays to drainage
🩺 Case 1 - Subacute Effusion
Malignancy-related effusion → gradual symptoms, large volume tolerated. 👉 Drain if symptomatic or haemodynamic compromise.
🩺 Case 2 - Acute Tamponade
Post-surgical patient with shock → echo confirms RA collapse. 👉 Immediate drainage + surgical involvement.
🩺 Case 3 - Anticoagulation-Related
DOAC → haemopericardium → tamponade. 👉 Reverse anticoagulation + urgent drainage.
📚 References
- 2015 ESC Guidelines for the diagnosis and management of pericardial diseases 👉 Gold-standard guideline for pericardial effusion, tamponade physiology, and management strategies European Society of Cardiology (ESC)
- Resuscitation Council UK – Advanced Life Support (ALS) Guidelines 👉 Covers obstructive shock, cardiac arrest, and emergency management principles including tamponade Resuscitation Council UK ALS
- NICE Clinical Knowledge Summary (CKS): Pericarditis 👉 UK primary care–focused guidance on causes, investigation, and initial management NICE CKS Pericarditis
- NICE Guideline NG158 – Acute coronary syndromes 👉 Relevant for post-MI complications (e.g. free wall rupture → tamponade) NICE NG158
- NICE Guideline NG51 – Sepsis 👉 Important differential when patients present with shock and raised inflammatory markers NICE NG51
- Oxford Handbook of Clinical Medicine (11th Edition) 👉 Concise bedside summary of tamponade signs (Beck’s triad, pulsus paradoxus) and management
- Kumar & Clark’s Clinical Medicine (10th Edition) 👉 Detailed pathophysiology of pericardial disease and haemodynamic compromise
- UpToDate – Cardiac tamponade 👉 Comprehensive, regularly updated review of diagnosis and treatment (subscription required) UpToDate
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery