Related Subjects: Asthma
|Acute Severe Asthma
|Exacerbation of COPD
|Pulmonary Embolism
|Cardiogenic Pulmonary Oedema
|Pneumothorax
|Tension Pneumothorax
|Respiratory (Chest) infections Pneumonia
|Fat embolism
|Hyperventilation Syndrome
|ARDS
|Respiratory Failure
|Diabetic Ketoacidosis
|Assessing Breathlessness
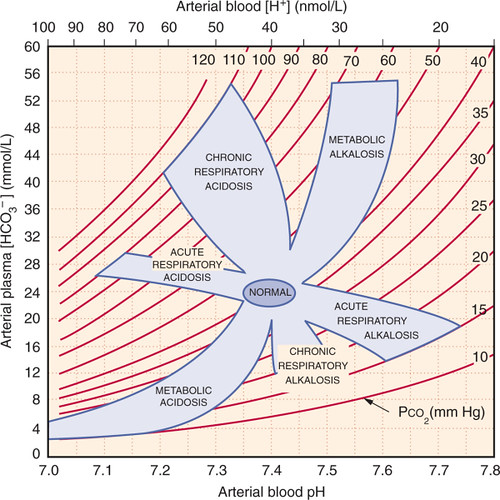
🩸 Analysis of Respiratory Alkalosis (ABG)
- 📈 pH: > 7.45 (alkalaemia)
- 🫁 PaCO₂: ↓ (primary abnormality)
- 🧪 HCO₃⁻: usually normal (acute) or ↓ (chronic renal compensation)
- 🌬️ PaO₂: often normal or mildly low if due to lung pathology
⚡ Aetiology
- Excessive ventilation → ↓ CO₂ → reduced carbonic acid → alkalosis
- Renal compensation develops slowly (↓ HCO₃⁻ reabsorption in chronic cases)
🦠 Causes
- 😰 Anxiety / Panic attacks → hyperventilation
- 🫀 Pulmonary embolism, asthma, pneumonia, pulmonary oedema
- 💊 Drugs & toxins: salicylate overdose, excessive diuretic therapy
- 🧠 CNS causes: stroke, head injury, fever
- 🫁 Hypoxia from high altitude or severe lung disease
- 🩸 Liver failure (stimulates central respiratory drive)
👀 Clinical Features
- 🌡️ Dizziness, light-headedness, tingling (perioral, fingers)
- 💪 Carpopedal spasm due to ↓ ionised calcium
- 🌀 Confusion, seizures if severe
💊 Management
- 🎯 Treat underlying cause (e.g., PE, infection, asthma)
- 🧘 Reassurance & breathing control for panic-related hyperventilation
- ⚠️ Paper bag breathing (to re-inhale CO₂) is no longer routinely advised in clinical settings due to safety concerns - reassurance and controlled breathing techniques are safer
- In chronic disease → manage hypoxia, correct underlying trigger
3 Clinical Cases - Respiratory Alkalosis 🌬️🫁
- Case 1 - Anxiety-induced hyperventilation 😰: A 26-year-old student presents to A&E with acute shortness of breath, chest tightness, and tingling in her hands and around her mouth during an exam panic attack. ABG: pH 7.54, PaCO₂ 3.0 kPa, HCO₃⁻ 22 mmol/L. Teaching: Anxiety and panic lead to over-breathing → ↓PaCO₂ → respiratory alkalosis. Symptoms include paraesthesia, dizziness, and carpopedal spasm from transient hypocalcaemia.
- Case 2 - Sepsis and tachypnoea 🦠: A 68-year-old woman admitted with pneumonia is febrile (39.2°C) and tachypnoeic (RR 32/min). ABG: pH 7.49, PaCO₂ 3.5 kPa, PaO₂ 8.5 kPa on air. Teaching: Early sepsis causes tachypnoea and hyperventilation → respiratory alkalosis, often mixed later with metabolic acidosis (septic shock). Always interpret ABG in clinical context.
- Case 3 - Pregnancy 🤰: A 30-year-old woman, 28 weeks pregnant, is noted to have mild tachypnoea at rest. Routine ABG: pH 7.47, PaCO₂ 3.8 kPa, HCO₃⁻ 20 mmol/L. Teaching: In normal pregnancy, progesterone stimulates central respiratory drive → mild chronic hyperventilation with compensated respiratory alkalosis. This facilitates maternal–fetal CO₂ transfer and is physiological, not pathological.
