Infectious Mononucleosis (EBV Most Often)
For individual viral causes, please see their dedicated sections. Infectious mononucleosis is a classic “exam syndrome” - always think EBV first, but don’t forget the mimics.
📖 About Infectious Mononucleosis
- A clinical syndrome usually caused by Epstein-Barr Virus (EBV), a gamma-herpesvirus that infects B lymphocytes.
- Other agents (e.g. CMV, HIV, HHV-6, toxoplasmosis) can cause an “EBV-like” illness and should be considered in differential diagnoses.
- EBV is linked to oncogenesis (Hodgkin’s lymphoma, Burkitt’s lymphoma, nasopharyngeal carcinoma).
📊 Epidemiology
- Most cases present in teenagers or young adults (“kissing disease”).
- In developing countries, infection often occurs in early childhood, where it tends to be mild or asymptomatic.
🦠 Spread
- Mainly transmitted through saliva (“kissing”, sharing utensils, droplets).
- Infects B lymphocytes via the CD21 receptor, leading to a marked T-cell response responsible for many symptoms.
🧾 Causes of Mononucleosis-like Illness
- EBV - most common.
- CMV - especially in adults with negative EBV tests.
- HHV-6/7 - less common.
- HIV seroconversion - important to rule out in high-risk cases.
- Toxoplasmosis - may mimic EBV but usually with exposure history (e.g. undercooked meat, cat litter).
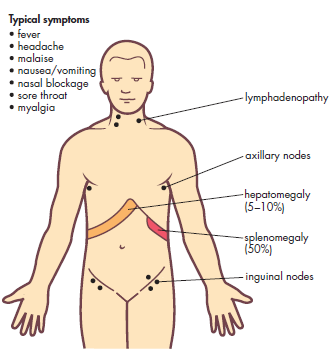
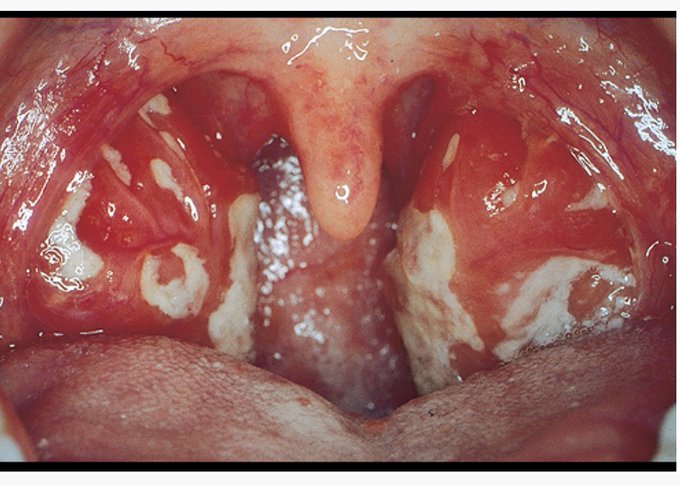
🩺 Clinical Presentation
- Classic triad: fever, sore throat, and posterior cervical lymphadenopathy.
- Splenomegaly (risk of rupture if trauma occurs) and hepatomegaly may be present.
- Ampicillin Rash: Use of ampicillin/amoxicillin in EBV infection produces a widespread maculopapular rash.
- Other features: profound fatigue, malaise, palatal petechiae.
- Severe manifestations: laryngeal oedema, cranial nerve palsies, meningoencephalitis, haemolytic anaemia, glomerulonephritis, myocarditis, or pneumonitis.
📉 Rare Long-Term Complications
- Hodgkin’s lymphoma
- Endemic Burkitt’s lymphoma (esp. Africa, linked with malaria co-infection)
- Nasopharyngeal carcinoma (esp. in Southeast Asia)
🔬 Investigations
- FBC: Lymphocytosis with >10% atypical lymphocytes is highly suggestive.
- Monospot (heterophile antibody) test: Quick bedside test but may be negative in first week of illness.
- EBV serology: IgM anti-VCA confirms acute EBV infection.
- Consider HIV testing if presentation is atypical or risk factors are present.
💊 Management
- Supportive: fluids, rest, paracetamol/NSAIDs, warm saline gargles.
- Steroids: Reserved for airway obstruction due to tonsillar hypertrophy or severe systemic complications.
- Avoid antibiotics unless bacterial superinfection suspected. Avoid ampicillin/amoxicillin (rash risk).
- Avoid contact sports for at least 4 weeks (or until splenomegaly resolves on exam/USS) due to risk of splenic rupture.
📝 Exam Pearls
- Teenager with sore throat, lymphadenopathy, hepatosplenomegaly, and rash after amoxicillin = EBV.
- Posterior cervical nodes are more typical of EBV, anterior cervical of strep throat.
- Always exclude HIV in mononucleosis-like illness with risk factors.
