
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
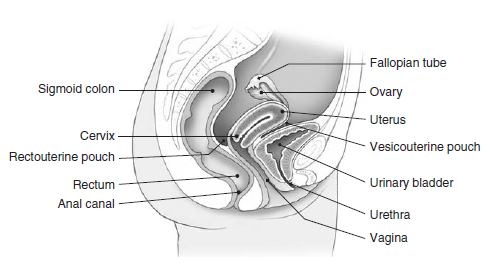
Pelvic Pain
💡 Pelvic pain is a common but complex symptom with gynaecological, urological, gastrointestinal, musculoskeletal, and even neurological causes. It may be acute (surgical emergency such as ectopic pregnancy or ovarian torsion) or chronic (endometriosis, interstitial cystitis). A structured approach is essential to avoid missing life-threatening pathology.
📝 Clinical History
- Site & Radiation: Localised (e.g., right iliac fossa in appendicitis) or diffuse. Radiation to back, thighs, or shoulder tip (ectopic rupture).
- Onset & Duration: Sudden (torsion, rupture) vs gradual (PID, endometriosis).
- Character: Cramping (dysmenorrhoea, IBS), sharp (torsion, ectopic), dull (fibroids).
- Associated Symptoms:
- Menstrual: heavy bleeding, dysmenorrhoea, missed period
- Urinary: dysuria, frequency, haematuria
- GI: constipation, diarrhoea, anorexia
- Gynaecological: vaginal discharge, dyspareunia, infertility
- Aggravating/Relieving Factors: Movement, urination, menstruation, intercourse.
- PMH: PID, endometriosis, surgeries, STIs, anticoagulation use.
- FH: Ovarian, bowel, or breast cancer (think hereditary syndromes).
🩺 Physical Examination
- General: Pallor, cachexia, fever, haemodynamic status.
- Abdomen: Distension, scars, masses, guarding, rebound.
- Pelvic exam:
- Speculum: discharge, cervical pathology
- Bimanual: uterine size, adnexal tenderness, cervical motion tenderness (PID)
- Other: CVA tenderness (renal colic), rectal exam if appendicitis/rectal mass suspected.
🔬 Investigations
- Bloods: CBC, CRP/ESR, β-hCG, renal & liver function, coagulation profile.
- Urine: Urinalysis, culture (exclude UTI).
- Microbiology: Cervical swabs for chlamydia/gonorrhoea if PID suspected.
- Imaging:
- Transvaginal + transabdominal ultrasound (first line)
- Doppler (suspect torsion)
- CT/MRI (complex cases, suspected malignancy, appendicitis/diverticulitis)
- Special: Diagnostic laparoscopy (endometriosis, uncertain cases).
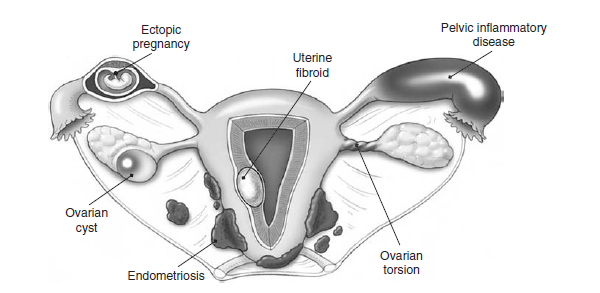
📊 Causes of Pelvic Pain
| Cause | Clinical Features | Diagnostic Tests | Management |
|---|---|---|---|
| 🤰 Ectopic Pregnancy | Acute pelvic pain, missed period, vaginal bleeding, shoulder tip pain if rupture | β-hCG ↑, TVUS: no intrauterine pregnancy | Methotrexate (stable, unruptured); laparoscopy (ruptured) |
| 🦠 Pelvic Inflammatory Disease | Bilateral pelvic pain, fever, discharge, dyspareunia, cervical motion tenderness | Cervical swabs, CBC ↑, USS ± tubo-ovarian abscess | Broad-spectrum antibiotics, hospitalise if severe, treat partner |
| ⛔ Ovarian Torsion | Sudden severe unilateral pain, nausea, vomiting, adnexal tenderness | USS with Doppler: ↓ blood flow | Emergency laparoscopy: detorsion or oophorectomy |
| 🌿 Endometriosis | Chronic pelvic pain, dysmenorrhoea, dyspareunia, infertility | USS (endometriomas), laparoscopy = gold standard | Hormonal therapy; laparoscopic excision; ART if infertility |
| 💥 Ovarian Cyst Rupture | Sudden unilateral pain, spotting, worsens with exertion | USS: free fluid, cyst remnants; CBC for blood loss | Analgesia; observe if stable; laparoscopy if unstable |
| ⚡ Appendicitis | RLQ pain, migrates from umbilicus, fever, N&V | CBC ↑ WCC; CT/USS = inflamed appendix | Appendectomy (laparoscopic preferred) |
| 💧 UTI | Suprapubic pain, dysuria, frequency, haematuria | Urinalysis, urine culture | Antibiotics; hydration |
| 🌸 Fibroids | Pelvic pressure, heavy bleeding, infertility | USS; MRI for large/complex fibroids | Hormonal therapy, myomectomy, hysterectomy |
| 🚻 Interstitial Cystitis | Chronic pelvic pain, urgency, frequency, relief after voiding | Urinalysis normal; cystoscopy (Hunner’s ulcers) | Bladder training; pentosan polysulfate; intravesical therapy |
⚠️ Red Flags
- Haemodynamic instability → ruptured ectopic, massive haemorrhage
- Fever + sepsis → tubo-ovarian abscess, perforated appendix
- Postmenopausal woman with new pelvic pain → malignancy
- Unexplained weight loss or ascites → ovarian cancer
💉 Management Principles
- Stabilise first: IV access, fluids, analgesia, resuscitate if unstable.
- Investigate while resuscitating: β-hCG, bloods, USS.
- Treat underlying cause: surgery for ectopic/torsion/appendicitis; antibiotics for PID/UTI; hormonal therapy for endometriosis/fibroids.
- Refer appropriately: gynaecology, general surgery, or urology.
🧑⚕️ Case Vignettes
Case 1: 👩 A 24-year-old woman with 6 weeks amenorrhoea presents with severe left iliac fossa pain and vaginal spotting. She collapses in the ED. ✅ Diagnosis: Ruptured ectopic pregnancy. ⚡ Immediate resuscitation, urgent laparoscopy.
Case 2: 👵 A 40-year-old woman with a history of infertility and dysmenorrhoea reports deep dyspareunia and chronic pelvic pain. TVUS shows a left “chocolate cyst.” ✅ Diagnosis: Endometriosis (endometrioma). 📌 Management: Hormonal suppression (OCP/GnRH agonist), laparoscopic excision, consider fertility support.
📚 References
- NICE NG88: Heavy Menstrual Bleeding & Pelvic Pain Guidelines
- RCOG GTG No. 21: Management of Acute Pelvic Pain in Women
- Kumar & Clark’s Clinical Medicine, 10th Ed.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery