🧠👁️👂 Susac's syndrome is a rare autoimmune microangiopathy affecting the
brain, retina, and cochlea.
💡 Always consider in young women with hearing loss + visual disturbance + encephalopathy.
Classical triad = 1) Sensorineural hearing loss, 2) Branched Retinal Artery Occlusions (BRAOs), 3) Encephalopathy.
📖 Introduction
- First described by John O. Susac in 1979.
- Autoimmune endotheliopathy causing microinfarctions in the cochlea, retina, and brain.
- Predominantly affects young women.
🔺 Classical Triad
- 🧠 Subacute encephalopathy.
- 👁️ Retinal arteriolar branch occlusions (BRAOs).
- 👂 Sensorineural hearing loss.
🧬 Aetiology / Pathology
- Microangiopathy with microinfarcts in cochlea, retina, corpus callosum.
- Corpus callosum = most frequently affected region.
- Possible role of anti-endothelial cell antibodies.
🔎 Clinical Features
- 🧠 Cognitive changes: headache, memory loss, personality change, confusion, seizures.
- 🚶 Ataxia, migrainous headaches, delirium.
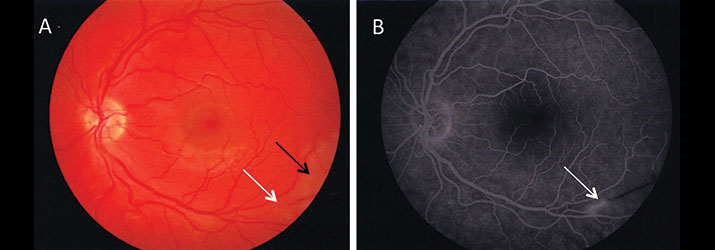
- 👁️ Acute visual loss from BRAOs.
- 👂 Asymmetric, bilateral sensorineural hearing loss (low-frequency loss).
- 📈 Typically monophasic, lasting 2–4 years; may relapse, especially in pregnancy.
🧪 Investigations
- 🧪 Bloods: Often normal (FBC, U&E, CRP).
- 💉 CSF: ↑ protein, mild lymphocytosis.
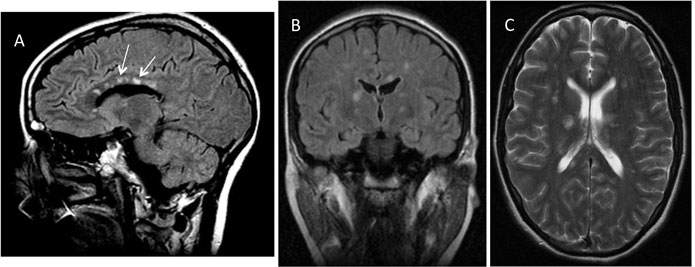
- 🧲 MRI: Pathognomonic findings:
- Central corpus callosum lesions ("snowball" lesions).
- “String of pearls” or “spoke lesions” along the callosal roof.
- Leptomeningeal enhancement (⅓ cases).
- 🌈 Fluorescein angiography: BRAOs.
- 🎧 Audiogram: Low-frequency sensorineural loss.
🖼️ Imaging Examples
⚖️ Differential Diagnoses
- Atypical MS or ADEM.
- CADASIL, SLE, APL syndrome, vasculitis.
- Neuro-Behçet’s disease.
- Lymphoma, temporal arteritis.
- Cogan’s syndrome (ocular + vestibuloauditory, no encephalopathy).
💊 Management
- 🎯 Immunotherapy (mainstay):
- IV methylprednisolone, then oral prednisolone taper.
- IVIG or plasmapheresis for refractory/active disease.
- Immunosuppressants: azathioprine, mycophenolate, rituximab, cyclophosphamide.
- 👂 Hearing loss: Intratympanic dexamethasone may give temporary relief.
- 🔄 Monitoring: Serial MRI, audiometry, and fluorescein angiography to track disease activity.
- 🧠 Course is usually self-limiting (2–4 yrs), but relapse prevention and close follow-up essential.
📚 References