
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Trauma: Resuscitative Thoracotomy
Related Subjects: |Initial Trauma Assessment and Management |Thoracic Trauma Assessment and Management |Flail Chest Rib fractures |Resuscitative Thoracotomy |Haemorrhage control |Traumatic Head/Brain Injury |Traumatic Cardiac Arrest |Abdominal trauma |Tranexamic Acid |Silver Trauma |Cauda Equina |Adult Resus:Basic Life Support |Adult Resus: Advanced Life Support |Resus:Acute Haemorrhage
Introduction
- 🫀 Resuscitative thoracotomy is a last-resort, life-saving procedure in catastrophic trauma, performed to restore circulation and control exsanguination.
- It should only be undertaken by trained and credentialed professionals (Emergency Physicians, trauma surgeons, cardiothoracic surgeons) in centres equipped for definitive care.
- ⚡ While ideally performed in theatre, if a patient loses cardiac output it must be carried out immediately in the Emergency Department.
Indications
🎯 Primary goals: relieve tamponade, decompress tension, control haemorrhage, restore circulation.
- 💨 Decompression of tension pneumothorax
- ❤️ Relief of pericardial tamponade
- 🪡 Repair of penetrating cardiac wounds
- 🩸 Control of intrathoracic haemorrhage
- ✋ Open cardiac massage
- 🔑 RCEM: within the scope of practice for trained Emergency Physicians in extremis.
✅ Absolute Indications: - Penetrating chest trauma with witnessed loss of output in ED. - Tamponade with cardiac arrest. - Exsanguinating thoracic haemorrhage.
❌ Contraindications: - No cardiac output for >10 mins without ROSC. - Asystole without pericardial tamponade. - Blunt trauma with cardiac arrest (unless tamponade strongly suspected).
Acute Management Protocol
- 📞 Call cardiothoracic support – notify consultant + SpR immediately.
- 🧰 Prepare thoracotomy kit – sterile instruments, suction, lighting, cardiac sutures.
- 🔍 Indications check – penetrating thoracic/upper abdominal trauma with arrest, or need for aortic cross-clamp in exsanguination.
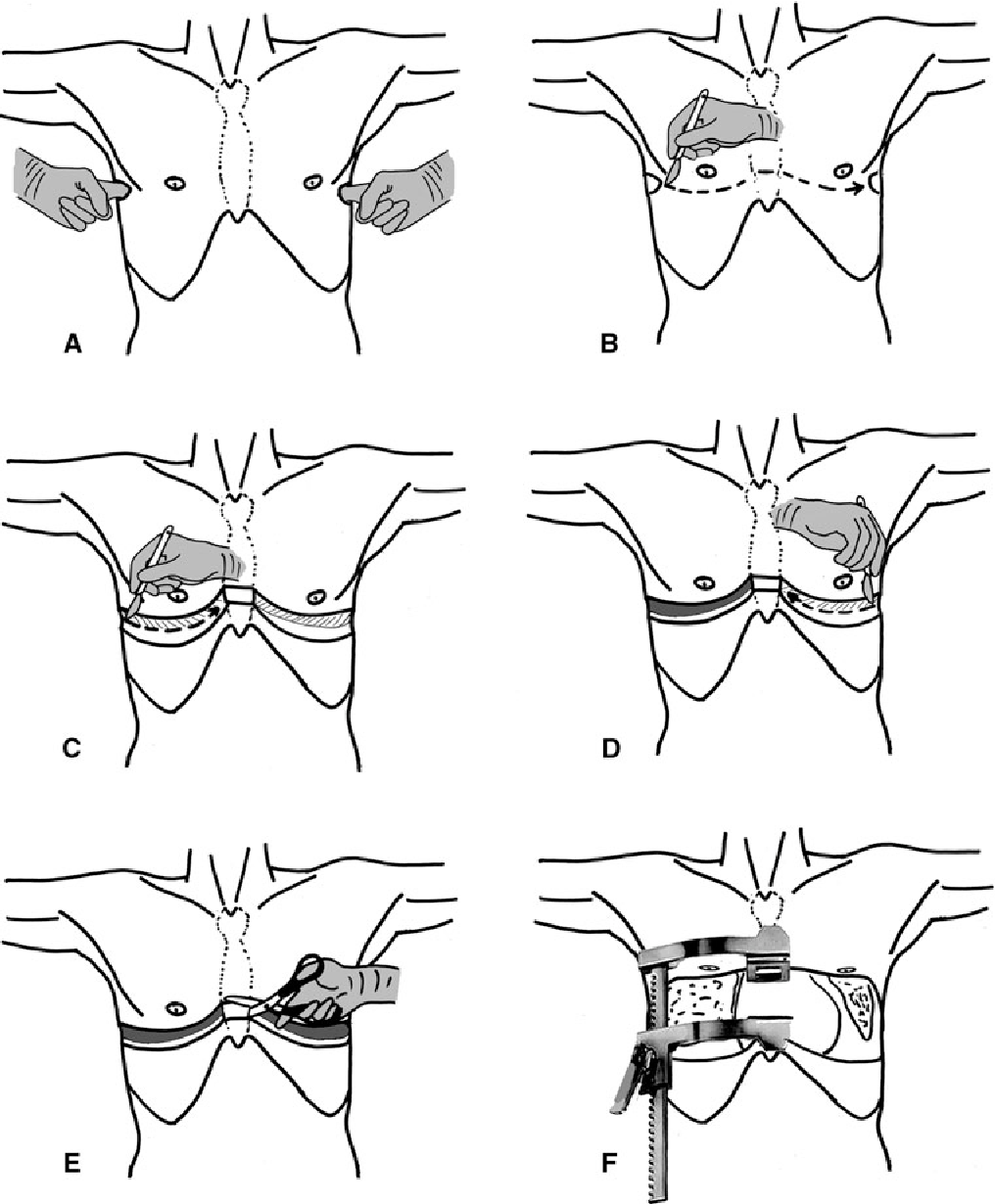
- ✂️ Bilateral thoracostomies – 5th intercostal space, mid-axillary line; decompress air/fluid before proceeding.
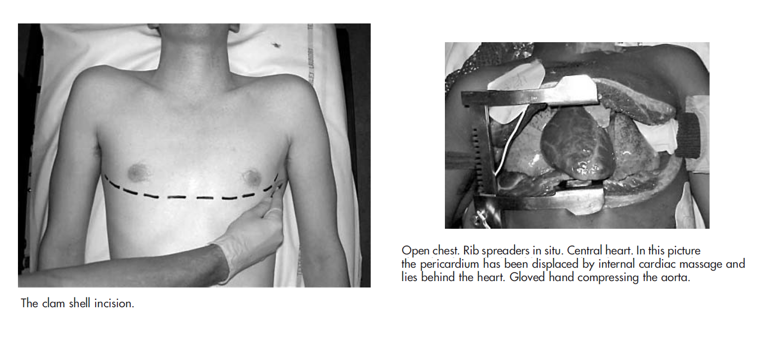
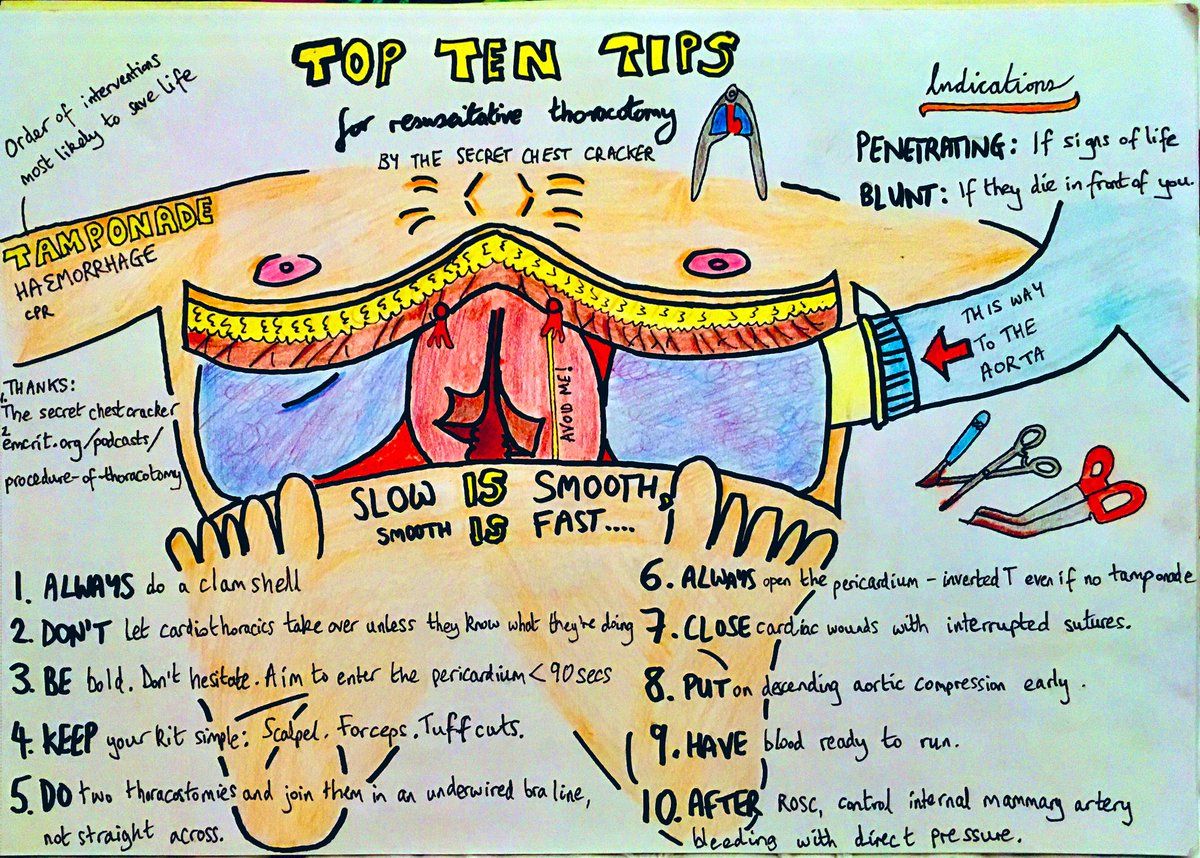
- 🔪 Clamshell incision – join thoracostomies across sternum (Tuff Cut scissors / Gigli saw).
- 🫀 Cardiac/pericardial management:
- Open pericardium longitudinally; evacuate blood/clot.
- Direct pressure or 4-0 Prolene sutures for cardiac wounds.
- Pack/Foley catheter for temporary tamponade.
- ⛓️ Control bleeding – clamp hilum/aorta if required.
- 🤲 Open cardiac massage if no spontaneous output.
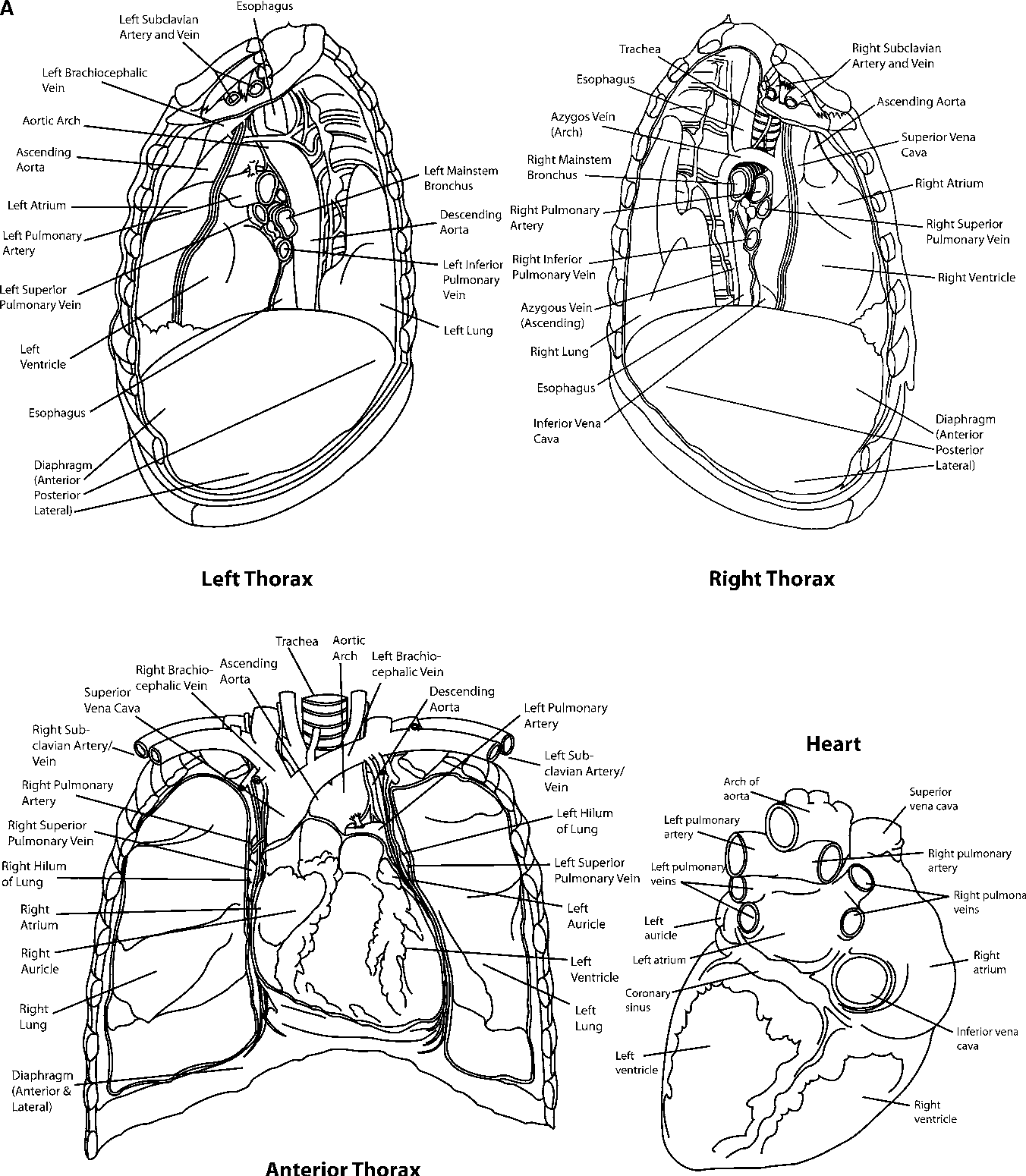
Relevant Anatomy
- ❤️ Heart + great vessels (aorta, pulmonary arteries, SVC/IVC)
- 🫁 Lungs & pleura (managing haemothorax/pneumothorax)
- 🪶 Diaphragm (injuries may extend to abdomen)
Surgical Approaches
- 🟧 Clamshell incision – gold standard ED approach; excellent bilateral access.
- 🟥 Left anterolateral thoracotomy – faster, for left-sided/cardiac access.
- ⬜ Median sternotomy – ideal in controlled theatre settings.
Post-Procedure Considerations
- 🩺 Stabilisation – haemostasis, volume resuscitation, secure airway/ventilation.
- 📉 Monitoring – haemodynamics, arrhythmias, re-bleeding.
- 📝 Documentation – timings, interventions, findings, patient response.
- 🚑 Transfer – to operating theatre or ICU for definitive management.
Outcomes
- 🔪 Penetrating cardiac trauma – survival up to 15–20% if performed promptly.
- 🚗 Blunt trauma – survival extremely poor (<2%).
- ⏱️ Outcome depends on time to thoracotomy, mechanism of injury, and availability of definitive surgical repair.
References
- Royal College of Emergency Medicine (RCEM) Guidelines
- NEJM Review: Resuscitative Thoracotomy
- Advanced Trauma Life Support (ATLS®) 10th Edition
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery