🧠 Cerebral Amyloid Angiopathy (CAA) = amyloid-β deposition in walls of small/medium cerebral vessels → fragility → recurrent lobar ICH.
💡 Suspect in age >70, lobar haemorrhage, normotensive, often with cognitive decline or “amyloid spells” (TIA-like).
📖 Introduction
- CAA is a common cause of spontaneous lobar intracerebral haemorrhage in elderly.
- Deposition occurs in leptomeningeal & cortical vessels, distinct from systemic amyloidosis (Pantoni 2010).
- Inflammatory variant (CAA-RI) can cause subacute deficits and is steroid-responsive (Moussaddy 2015).
⚙️ Aetiology & Genetics
- Amyloid-β fibril deposition in small cortical/leptomeningeal arteries.
- Often coexists with Alzheimer’s, but not all CAA patients have dementia.
- Genetics: ApoE ε2/ε4 alleles; rare familial forms – Dutch type (APP mutation, midlife lobar ICH ± dementia), Icelandic type (Cystatin C mutation, brainstem/cerebellar involvement).
🔬 Pathology
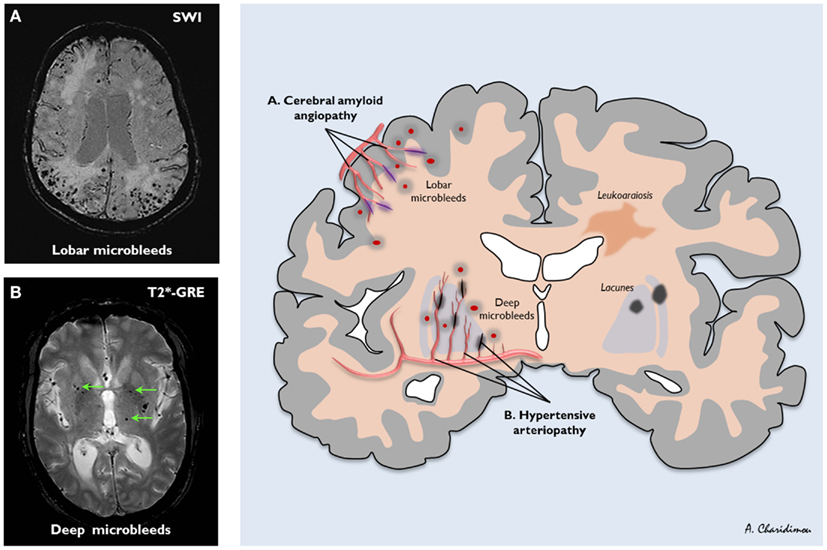
- Lobar haemorrhage (temporal/occipital > frontal/parietal), sparing deep nuclei (contrast with hypertensive bleeds).
- Microscopy: β-amyloid in media & adventitia; Congo red +ve.
- CAA-RI: inflammatory infiltrates, oedema on MRI, steroid-responsive.
🩺 Clinical Features
- Acute lobar ICH → headache, focal neurological deficits, seizures, coma in severe cases.
- “Amyloid spells” = transient, TIA-like deficits from small cortical bleeds.
- Recurrent micro/macrobleeds, sometimes provoked by minor trauma or antithrombotic therapy.
- Progressive cognitive decline if multiple haemorrhages.
🖼️ Imaging & Investigations
- CT: Acute lobar ICH; may recur in different lobes; deep nuclei spared.
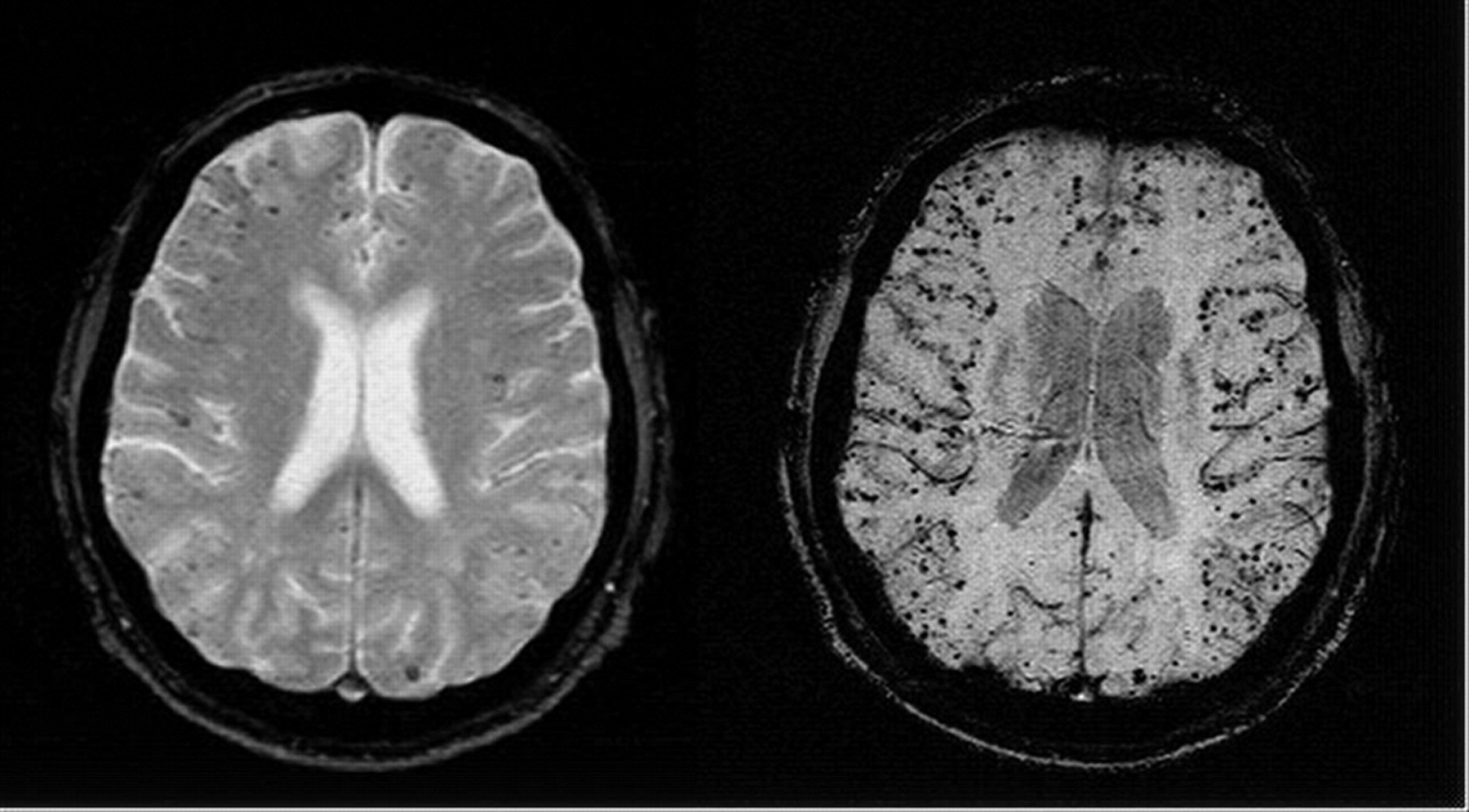
- MRI T2*/GRE/SWI: Microbleeds (<10 mm), cortical superficial siderosis, white matter changes.
- CAA-RI: T2 MRI shows oedema; often steroid-responsive.
- CTA/MRA: Exclude vascular malformations or venous sinus thrombosis.
- PET: Research only; amyloid imaging.
- Genetics: ApoE typing or APP/Cystatin C for suspected familial cases.
- Histology: Congo red staining post-mortem or biopsy confirms amyloid.
🧾 Boston Criteria (Revised)
| Category | Definition |
|---|
| Definite | Post-mortem: lobar haemorrhage + severe CAA, no other cause. |
| Probable with pathology | Lobar haemorrhage + biopsy/haematoma specimen showing amyloid, no other cause. |
| Probable | Age >60, multiple lobar bleeds on imaging, no other cause. |
| Possible | Age >60, single lobar bleed, no other cause. |
🚩 Differentials
- Hypertensive deep bleed
- Lobar extension from putaminal ICH
- Haemorrhagic infarct transformation
- AVM or haemorrhagic tumour
- Venous sinus thrombosis
📉 Complications
- Recurrent ICH
- Seizures
- Hydrocephalus (rare)
- Dementia (stepwise or progressive)
- Inflammation
💊 Management (Guideline-Aligned)
- ⚠️ Avoid antiplatelets, anticoagulants, thrombolysis if possible – high risk of recurrent lobar ICH (AHA/ASA 2022; NICE NG128).
- Standard acute haemorrhagic stroke care:
- BP control: target SBP ~130–150 mmHg acutely; long-term <140/90 mmHg.
- ICP management and supportive care.
- Seizure prophylaxis if indicated.
- Multidisciplinary stroke unit care.
- Falls prevention and trauma reduction.
- Surgery only for life-threatening haematoma or hydrocephalus.
- CAA-RI: steroids for inflammatory variant.
- Long-term: cognitive support, seizure management, lifestyle optimisation (BP, diet, exercise, limit alcohol, avoid smoking).
📖 Guideline Evidence
- International CAA/WORLD STROKE ORGANIZATION (2025): Diagnosis, risk stratification, antithrombotic avoidance, CAA-RI management.
- AHA/ASA 2022 Spontaneous ICH Guideline: Acute BP lowering, imaging-based risk assessment, stroke unit care.
- UK NICE Stroke Guidance NG128: Acute ICH care, BP control, stroke unit admission, MDT management.
- Radiopaedia – Imaging pearls
🖼️ Example Imaging
💡 Exam Pearls
– Age >70 + lobar ICH + normotension → think CAA.
– MRI T2*/GRE/SWI → detect microbleeds (“pepper pot cortex”).
– Avoid anticoagulation unless absolutely necessary; consider specialist review.
– CAA-RI variant → steroid-responsive; acute BP control crucial.
– Recurrent lobar bleeds and stepwise cognitive decline suggest advanced disease.
📚 References
