Related Subjects:
|Atherosclerosis
|Ischaemic heart disease
|Assessing Chest Pain
|ACS - General
|ACS - STEMI
|ACS - NSTEMI
|ACS - GRACE Score
|ACS - ECG Changes
|Cardiac Troponins
|ACS - Post MI arrhythmias
|ACS: Right Ventricular Infarction
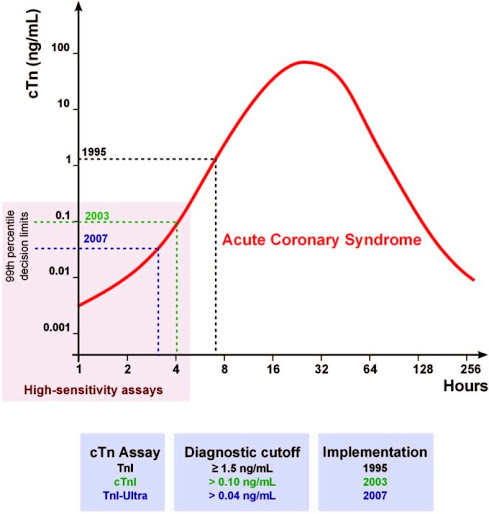
⏱️ Timing update: After myocardial injury, high-sensitivity troponin (hs-cTn) typically rises within ~1–3 h, peaks at ~12–24 h, and stays elevated for 7–14 days. (It does not rise “within minutes”).
🧪 Sampling: Use your lab’s validated pathway (0/1 h or 0/2–3 h). If not available, use 0 h + 3–6 h (extend to 12 h if symptoms very recent).
📖 About
- Troponin controls actin–myosin contraction; clinically we measure cTnI and cTnT (not TnC).
- Even tiny necrosis (~1 g myocardium) can be detected with modern hs-assays.
🩺 When and Why to Test
- Indicated if ACS suspected: ischemic chest pain, dyspnoea, syncope/collapse, concerning ECG.
- Use hs-cTn within a structured 0/1 h or 0/2–3 h pathway + clinical/ECG correlation.
📜 Universal Definition of MI (4th)
- Acute myocardial injury: cTn above the 99th percentile with rise/fall.
- Myocardial infarction (MI): acute injury + ischemia evidence (symptoms, ischemic ECG, imaging wall motion loss, or thrombus).
- Differentiate:
- Type 1 MI = plaque rupture/erosion.
- Type 2 MI = supply–demand mismatch (e.g., sepsis, anaemia, tachyarrhythmia).
📊 Interpretation (always assay-specific!)
- 99th percentile (URL): sex- and lab-specific. (e.g. Roche hs-cTnT ~14 ng/L).
- Delta (change): A significant rise/fall over 1–3 h = acute injury. Thresholds vary by assay ➝ check lab policy.
🛠️ Practical Pathway (if ECG not diagnostic)
- 0/1 h:
✔ Rule-out if very low baseline + tiny 1-h delta.
✔ Rule-in if high baseline or large 1-h delta.
❓ Otherwise ➝ observe to 2–3 h.
- 0/3–6 h (legacy): No rise by 3–6 h → MI unlikely. Persisting symptoms/ECG changes → continue work-up.
- Combine with risk scores (GRACE, HEART) for admission vs early outpatient testing.
📌 Example (values vary by assay!)
- 🟢 Normal/Low: hs-cTn below URL ≥3 h post-symptoms + tiny delta → rule-out MI.
- 🟡 Intermediate: Borderline elevation/small delta → repeat at 2–3 h, consider imaging/observation.
- 🔴 High/Probable MI: Clearly >URL with significant rise + ischemic features → treat as ACS.
⚠️ Non-ACS Causes of Troponin Rise
- ❤️ Cardiac: HF, tachy/bradyarrhythmias, myocarditis/pericarditis, HCM, valve disease, dissection, cardiac contusion/procedures, drugs (chemo).
- 🫁 Vascular/Respiratory: PE, severe pulmonary HTN, hypoxia.
- 🌍 Systemic: Sepsis/SIRS, stroke/SAH, renal failure (chronically raised), DKA, COPD exacerbation.
📒 Reporting & Pearls
- 🚫 Troponin ≠ MI alone → always use history, ECG, exam, imaging.
- 📉 Chronic elevation (e.g., CKD) without rise/fall = chronic injury.
- ♀ Use sex-specific cut-offs if validated.
- 🕒 Always document symptom onset time – it alters rule-out validity.
- ❌ Avoid CK-MB/myoglobin in hs-cTn era – little added value.
📈 Biomarker Timelines
| Marker | Rise | Peak | Normalises | Notes |
|---|
| hs-Troponin I/T | 1–3 h | 12–24 h | 7–14 d | Biomarker of choice |
| CK-MB | 3–8 h | ~16 h | 2–3 d | Rarely needed now |
| Myoglobin | 2–4 h | <12 h | ~24 h | Very early but non-specific |
| LDH | ~12 h | ~48 h | ~14 d | Nonspecific; historical |
💡 Safety tips:
🔴 If symptoms/ECG scream ischemia → treat & escalate regardless of a low first troponin.
📏 Always use your hospital’s assay-specific cut-offs and delta rules.
♻️ Repeat testing + clinical judgment = safest strategy.
