
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Rabies
Related Subjects: |Herpes Varicella-Zoster (Shingles) Infection |Chickenpox Varicella Infection |Varicella Cerebral Vasculopathy |Herpes Viruses |Herpes Zoster Ophthalmicus (HZO) Shingles |MonkeyPox |Mumps |Measles |Rubella (German Measles) |Epstein-Barr Virus infection |Cytomegalovirus (CMV) infections |CMV retinitis infections |Toxoplasmosis
🇮🇳🦠 India accounts for ~36% of global rabies deaths. 😢 Around 20,000 Indians die every year from rabies. 🐶 99% are transmitted by dogs. ☠️ Once symptoms start → fatality approaches 100%. 💉✅ If vaccination is taken on time → disease is almost 100% preventable.
⚠️📢 Public health advice is key.
🚫 Do not dismiss a bite because “it’s my pet”.
🚫⏳ Do not wait to “observe the dog first”.
🚫🩸 Do not judge risk by size of wound or absence of bleeding.
🚫💉 Do not rely only on the dog’s vaccination status.
- ⚠️ Early presentation for medical help makes a huge difference in outcome
- 🧴 Clean wound thoroughly with soap & water for at least 15 minutes.
- 💉 Start PEP immediately: rabies vaccine + rabies immunoglobulin (RIG) infiltrated into wound if indicated.
- ⚠️ Late symptomatic rabies → focus on palliative care, as 100% fatal once symptoms appear.
📖 About
- 🦠 Rabies is a zoonotic viral disease that primarily affects the CNS.
- 🌍 Rare in the UK and absent in Australia, but common in Asia & Africa.
- 🐕 Reservoirs: dogs (most common worldwide), bats, raccoons, and wild animals.
- Transmission via bites, scratches, or saliva contacting broken skin/mucosa.
🧬 Aetiology & Pathogenesis
- Caused by single-stranded RNA Lyssavirus (Rhabdoviridae family).
- 🎯 Infects local muscle cells → binds to nicotinic acetylcholine receptors at NMJs.
- 📡 Travels via retrograde axonal transport into CNS.
- Spreads to brain → salivary glands → allows host-to-host transmission.
🩺 Clinical Presentation
- ⏱️ Incubation: 1 week–1 year (typically 20–90 days).
- Prodrome: fever, headache, malaise, tingling/itching at bite site.
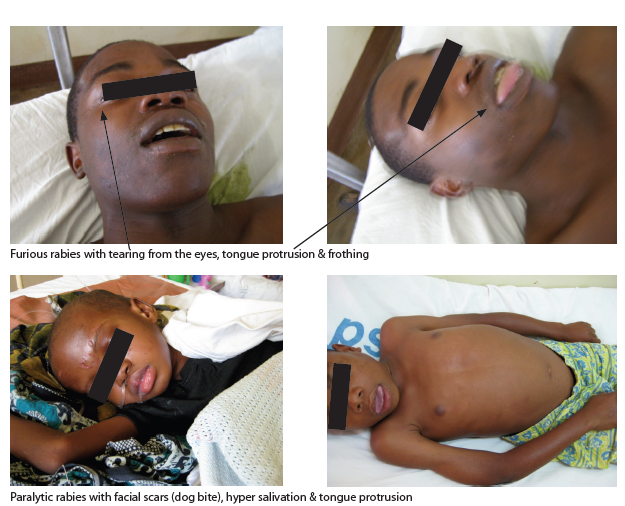
- Encephalitic (furious) rabies (80%):
- Agitation, delirium, ataxia, bizarre/aggressive behaviour.
- 💧 Hydrophobia: pharyngeal spasms on swallowing liquids.
- Hypersalivation, dilated pupils, myoclonus, priapism.
- Paralytic rabies (20%):
- Flaccid paralysis starting locally, mimics Guillain–Barré.
- ➡️ Progresses to coma, seizures, arrhythmias, DIC, death.
🔎 Investigations
- 🩸 Serology: neutralising antibodies (often negative early).
- 💉 CSF: mild ↑WCC, ↑protein.
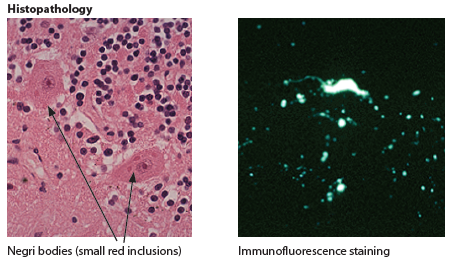
- 🧠 Histology: Negri bodies in hippocampus & Purkinje cells.
- 🔬 Skin biopsy: rabies antigen in hair follicle base.
- 🧪 PCR: detects viral RNA in saliva, CSF, or tissue.
💊 Management
- Once symptomatic: Almost universally fatal → palliative care only.
- PEP (Post-Exposure Prophylaxis):
- Immediate wound washing with soap & water (≥15 minutes).
- Rabies vaccine series (active immunity, effective in 7–10 days).
- Rabies Immunoglobulin (RIG) infiltrated into wound → passive immediate protection (t½ ≈ 21 days).
- 🤰 Pregnancy: Vaccine & RIG are safe.
- 🐕 If possible: euthanize & test offending animal brain tissue (Negri bodies/PCR).
- Hydrophobia, agitation, or coma → comfort measures & palliation.
⚠️ Complications
- Neurological failure → seizures, coma, brainstem dysfunction.
- Autonomic storm → hypersalivation, arrhythmias, temperature instability.
- Death usually from cardiorespiratory failure within 2–10 days of symptoms.
💡 Exam Tip: - Think rabies in a traveller returning from Asia/Africa with neurological symptoms + hydrophobia. - PEP = vaccine + RIG → start before symptoms develop. - Once symptoms start → universally fatal → palliation only.
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery