Sigmoid and Caecal Volvulus Adults
Related Subjects:
Small Bowel Obstruction
|
Colonic (Large Bowel) Obstruction
|
Small Bowel Ischemia
|
Hartmann's Procedure
|
Sigmoid and Caecal Volvulus
|
Acute Colonic Pseudo-obstruction
🔄 Volvulus is a leading cause of acute colonic obstruction in adults.
🚑 Emergency endoscopic decompression, detorsion, and reduction (EDDR) aim to decompress the dilated colon and untwist it.
✅ EDDR is the treatment of choice in uncomplicated patients.
📖 About
- ⚠️ A common cause of large bowel obstruction, particularly in older adults.
- Accounts for up to 5–10% of intestinal obstructions in Western countries, but much higher in endemic regions (e.g., South America, Africa).
🧬 Aetiology & Pathophysiology
- 🔁 Redundant sigmoid colon with a narrow mesenteric base predisposes to twisting.
- 🌀 "Volvulus" (Latin volvere) = to roll or twist around its axis.
- Leads to luminal obstruction ± vascular compromise → risk of ischaemia, gangrene, and perforation.
- Sigmoid colon most common; caecal volvulus less frequent but often more severe.
🤝 Associations
- 👴 Age 60–70 years, more common in men (M:F ≈ 2:1).
- 🧠 Neurological conditions: Parkinson’s disease, Multiple Sclerosis (MS).
- 💩 Chronic constipation, laxative abuse, psychiatric illness.
- 🌽 High-fibre diet, Chagas disease (in endemic regions).
🩺 Clinical Presentation
- 🚫 Constipation (intermittent or absolute).
- 😖 Colicky abdominal pain + progressive distension.
- 🤢 Nausea, vomiting, ± faeculent discharge.
- 🛑 Can progress to obstruction → peritonitis if perforated.
- 📜 40–60% report recurrent prior episodes ("chronic volvulus").
🔍 Investigations
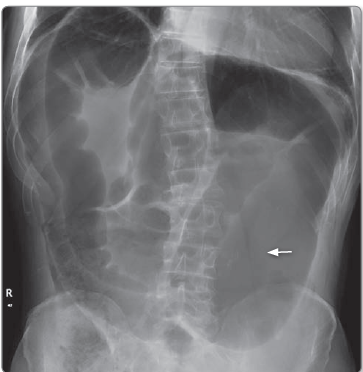
- 📸 Abdominal X-ray (AXR): "Coffee-bean sign" = massively dilated sigmoid loop pointing to the right upper quadrant.
- 🖥️ CT Scan: Highly sensitive - shows "whirl sign" of twisted mesenteric vessels.
- 🦆 Barium enema: "Bird’s beak" appearance at the point of torsion. Contraindicated if ischaemia/strangulation suspected.
Sigmoid volvulus
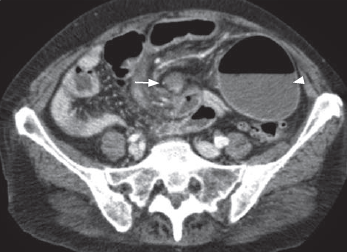
Caecal Voluvus
Axial CT post-contrast demonstrates the classic ‘swirl’ appearance of
the mesentry in caecal volvulus (arrow). The caecal pole is lying on the left of the
abdomen (arrowhead).
⚕️ Management
- Initial: ABC resuscitation, IV fluids, NBM, correct electrolytes, analgesia, NG tube if vomiting.
- Sigmoid Volvulus:
🌬️ Flexible sigmoidoscopy with rectal tube decompression (successful in ~70–90%).
⏱️ Leave flatus tube for 24–48h to prevent immediate recurrence.
🔁 High recurrence rate (40–50%) → elective sigmoid colectomy often advised after stabilisation.
🚨 If peritonitis, ischaemia, or failed endoscopy → emergency laparotomy ± resection (mortality up to 25%).
- Caecal Volvulus:
❌ Endoscopic decompression rarely effective.
🔪 Surgical approach: caecostomy or right hemicolectomy if gangrenous.
⚡ Mortality higher due to delayed diagnosis.
📚 References
